
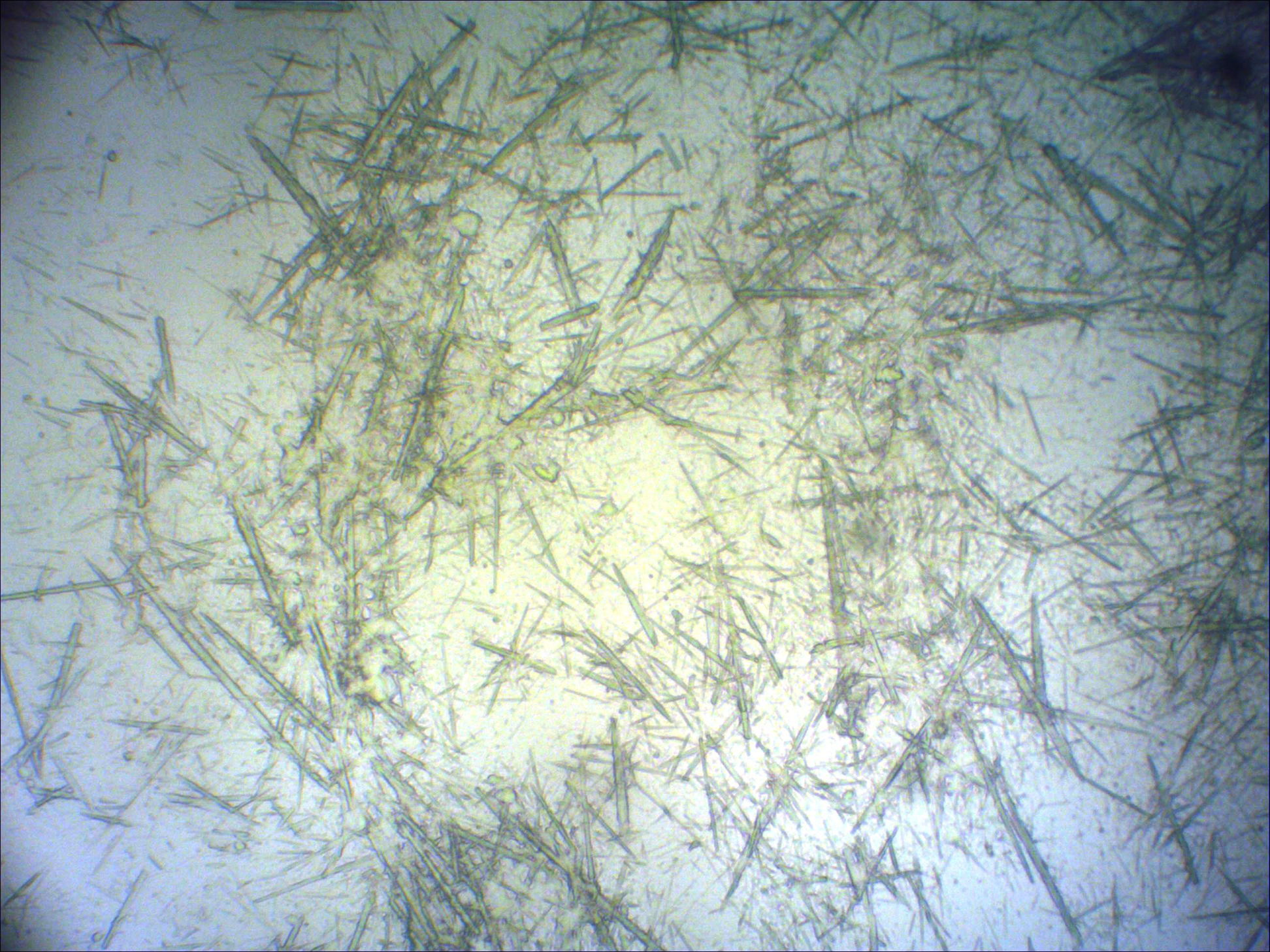
Figure 2. Fine needle aspiration cytology of a nodule showed negatively birefringent, needle-shaped crystals of monosodium urate.
Gout is a common rheumatologic condition of recurrent polyarticular involvement. Tophi may be the first sign of the disease. We report a 55-year-old hypertensive, chronic alcoholic and diabetic male with a three-year history of multiple painful skin-colored nodules on the forearms, elbows, feet, posterior thighs, and popliteal fossa associated with discharging sinuses. Serum uric acid was 8.1 mg/dL (normal: 2-7.4 mg/dL). Fine needle aspiration cytology showed monosodium urate crystals, which are pathognomonic for gout, confirmed histopathalogically.
A 55-year-old hypertensive, chronic alcoholic and diabetic male, presented with a three-year history of multiple painful skin-colored nodules with discharging sinuses on the forearms, elbows, feet, posterior thighs, and popliteal fossae (Figure 1).
|
|
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Painfull skin colored hyperpigmented nodules over posterior thigh Figure 2. Fine needle aspiration cytology of a nodule showed negatively birefringent, needle-shaped crystals of monosodium urate. |
|
Cutaneous examination revealed tender skin-colored to erythematous, firm nodules on forearm, elbows, feet, posterior thighs, and popliteal fossae. The lesions over the feet showed central softening with a few sinuses discharging chalky white material. Systemic examination was normal. X rays of elbows, wrists, knees, ankles, and bilateral great toes showed joint space reduction associated with bony destruction. Polarizing microscopy of fine needle aspiration cytology from a nodule showed multiple refractile crystals (Figure 2). The histopathology of a nodule (Figures 3 and 4) confirmed gout.
 |
 |
| Figure 3 | Figure 4 |
|---|---|
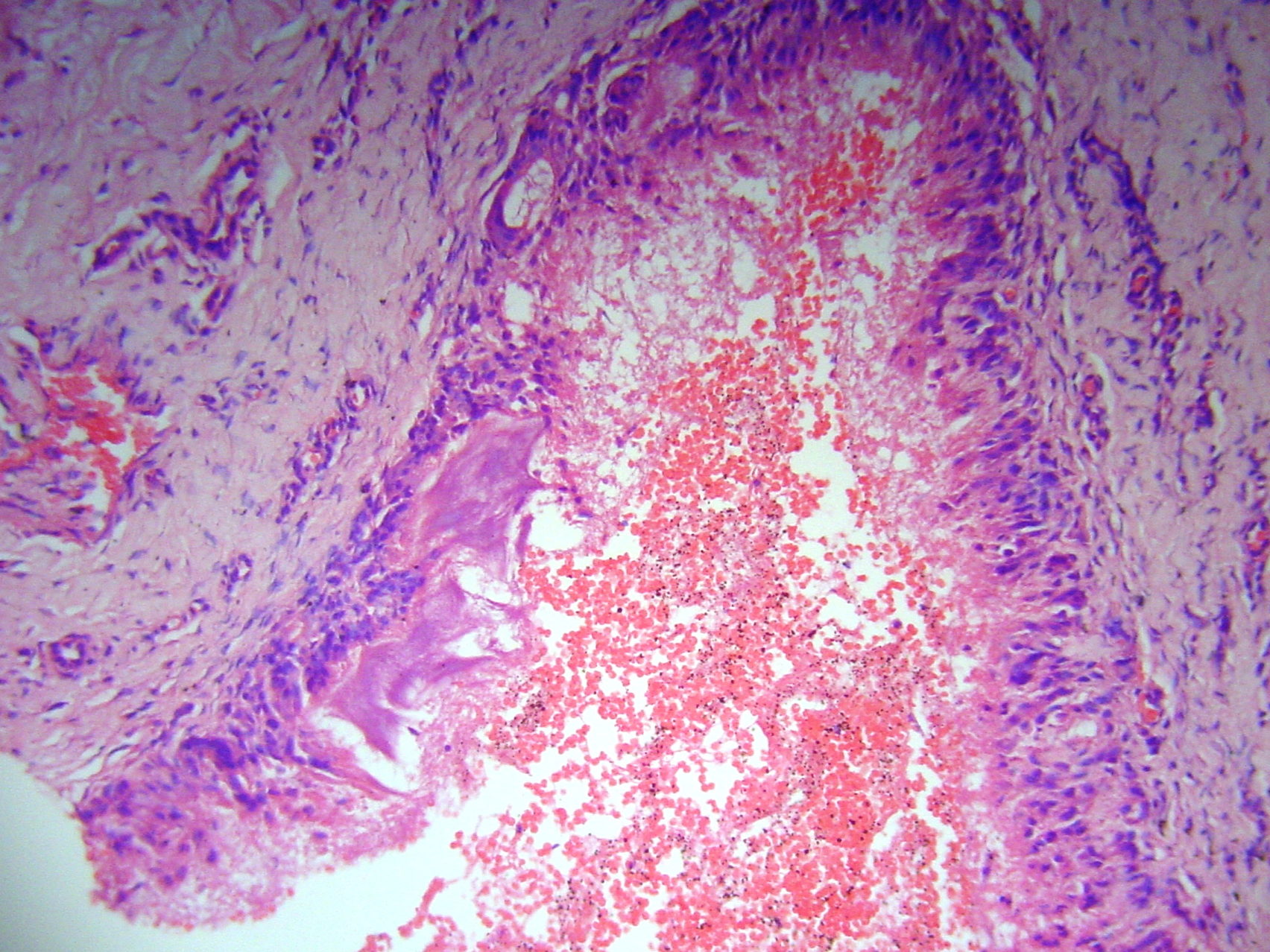
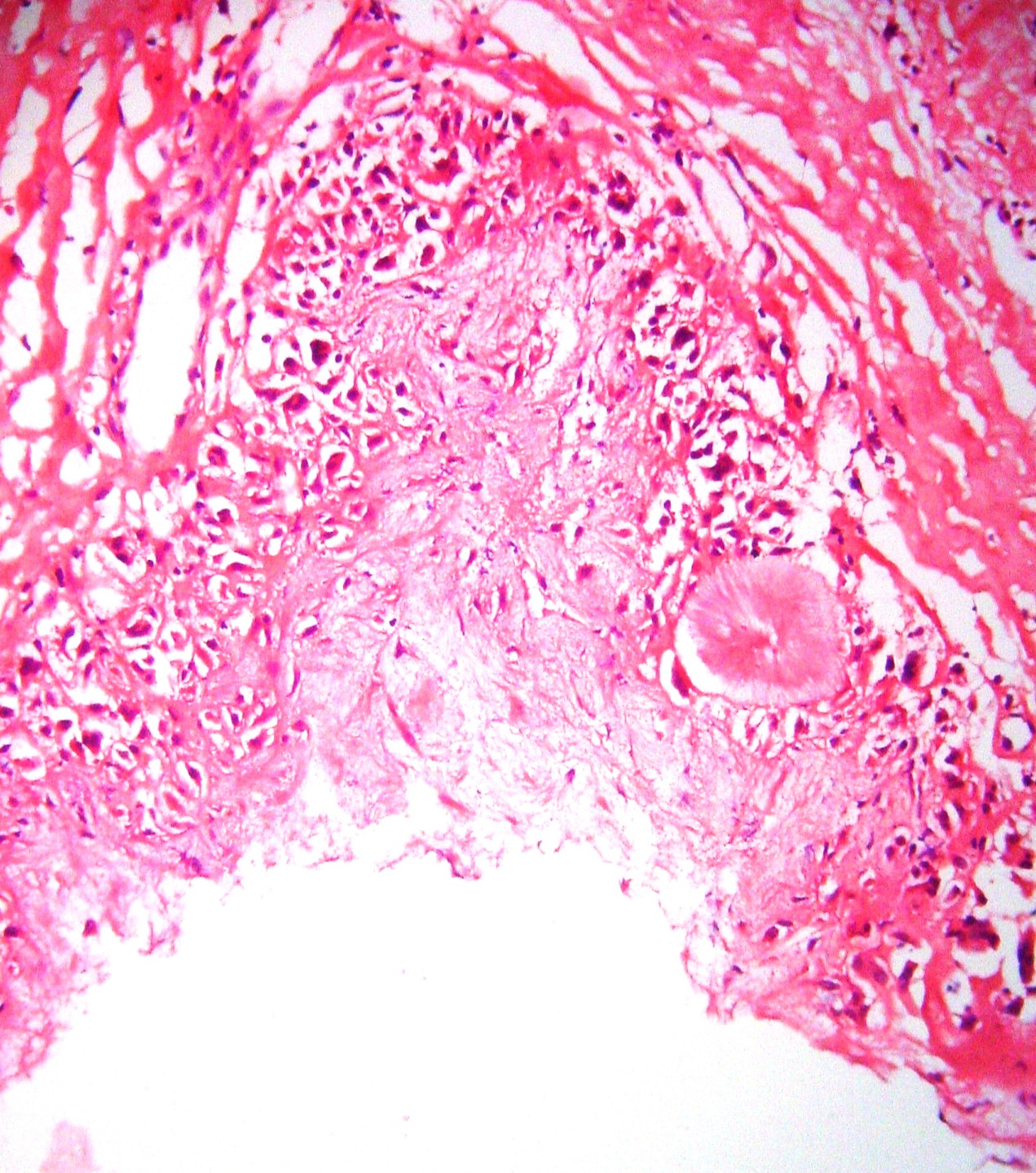
| Figure 3. Hematoxylin and eosin-stain showed multinucleated giant cells surrounding the urate deposits in the dermis. Figure 4. Hematoxylin and eosin-stain showed deposits of urate crystals in the reticular dermis that have a radial array and needle like clefts. |
|
Histopathology (hematoxylin and eosin) showed palisading granuloma involving the dermis. Fine needle aspiration revealed negatively birefringent, needle-shaped crystals of monosodium urate (MSU). Serum uric acid was 8.1 mg/dL (normal: 2-7.4 mg/dL), which helped in confirming the diagnosis of gout.
Ultrasound of the abdomen and pelvis was normal. Serum levels of calcium, phosphate, urea, creatinine, albumin, electrolytes, parathyroid hormone, and thyroid - stimulating hormone were within normal limits. The patient was started on colchicine, NSAIDs, and oral hypoglycemic and antihypertensive medications. After starting treatment, the pain improved with partial regression of the lesions.
Gout is characterized by deposition of monosodium urate monohydrate crystals in synovial fluid and joints, with or without hyperuricemia, renal disease, and nephrolithiasis. It is also known as podagra when it involves the big toe [1]. The four phases of gout include asymptomatic hyperuricemia, acute gouty arthritis, intercritical gout, and chronic tophaceous gout. Population studies suggest that the disorder is multifactorial and attributable to a combination of genetic and non-genetic factors [2]. The peak incidence occurs at 30 to 50 years, with male predominance. Women often do not develop gout until they reach menopause, when the uricosuric action of estrogens is lost [3].
The disease usually becomes symptomatic in the fourth to sixth decades when the first attack of acute gouty arthritis occurs. Recurrent, self-limiting attacks usually follow after a period of about 6 months to 2 years. Initially, only one joint may be affected, but in subsequent attacks other joints may be involved as well. If not properly treated, tophi develop an average of about 10 years after the onset of the disease. Tophi clinically present as subcutaneous nodules in the antihelix of the ear, olecranon, fingertips, cornea, aorta, or central nervous system. In a few reported cases, tophi break through the skin and appear as yellowish-white chalky nodules. For making the diagnosis of gout American College of Rheumatology (ACR)/Wallace criteria is commonly used. The gold standard for diagnosis is the demonstration of urate crystals in synovial fluid or in a tophus by polarized light microscopy [4]. The incidence of gout correlates strongly with serum urate concentrations, increasing markedly when these exceed 480 µmol/L (8.0 mg/dL) [5].
Under a polarization microscope crystals appear as brownish birefringent intra- and extracellular needles, 10 to 20 µm in length. For the histological examination of tophi, fixation in absolute ethanol is preferable, because formalin dissolves the characteristic crystals, leaving only amorphous material. The aggregate of urate crystals are often surrounded by palisaded granulomata [6]. Acute gout can be managed with NSAIDs, whereas chronic gout is managed by administration of probenecid, colchicine, and allopurinol. Patients should rest the affected joints until the acute attack subsides.
© 2011 Dermatology Online Journal