

Figure 2. Several pinhead-sized, slightly elevated, discrete, hypopigmented papules on the elbow.
A healthy 3-year-old boy came to our department for a linear asymptomatic eruption that had been present since he was born. He had been unsuccessfully treated with topical steroids. On physical examination, we found numerous tiny whitish flat-topped papules on the anterior trunk with a linear distribution and a few similar lesions on the elbows. The oral mucosa, palms, soles, and nails were spared.
|
|
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Numerous tiny papules with a linear distribution are present on the anterior trunk. Figure 2. Several pinhead-sized, slightly elevated, discrete, hypopigmented papules on the elbow. |
|
 |
 |
| Figure 3 | Figure 4 |
|---|---|
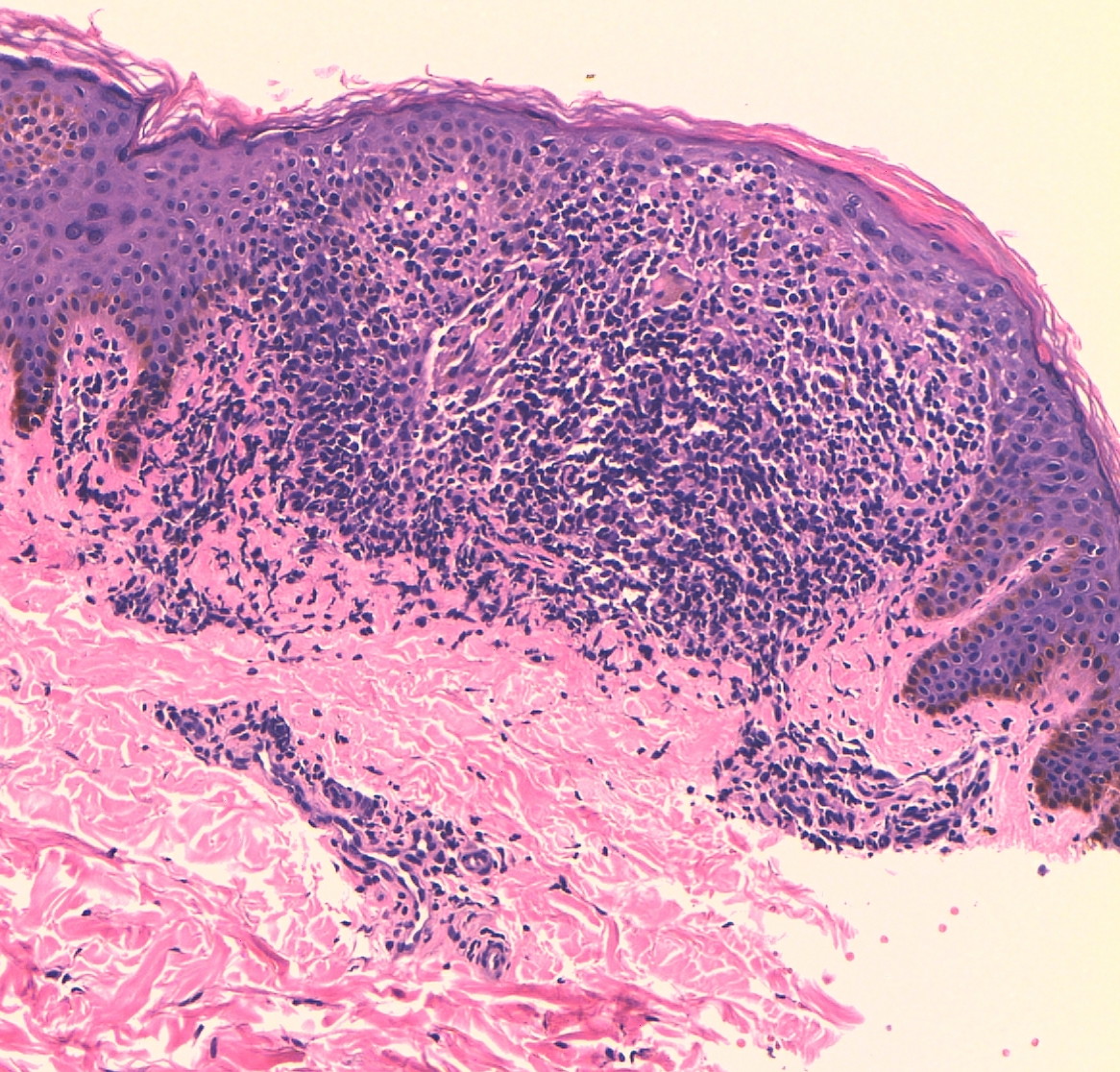
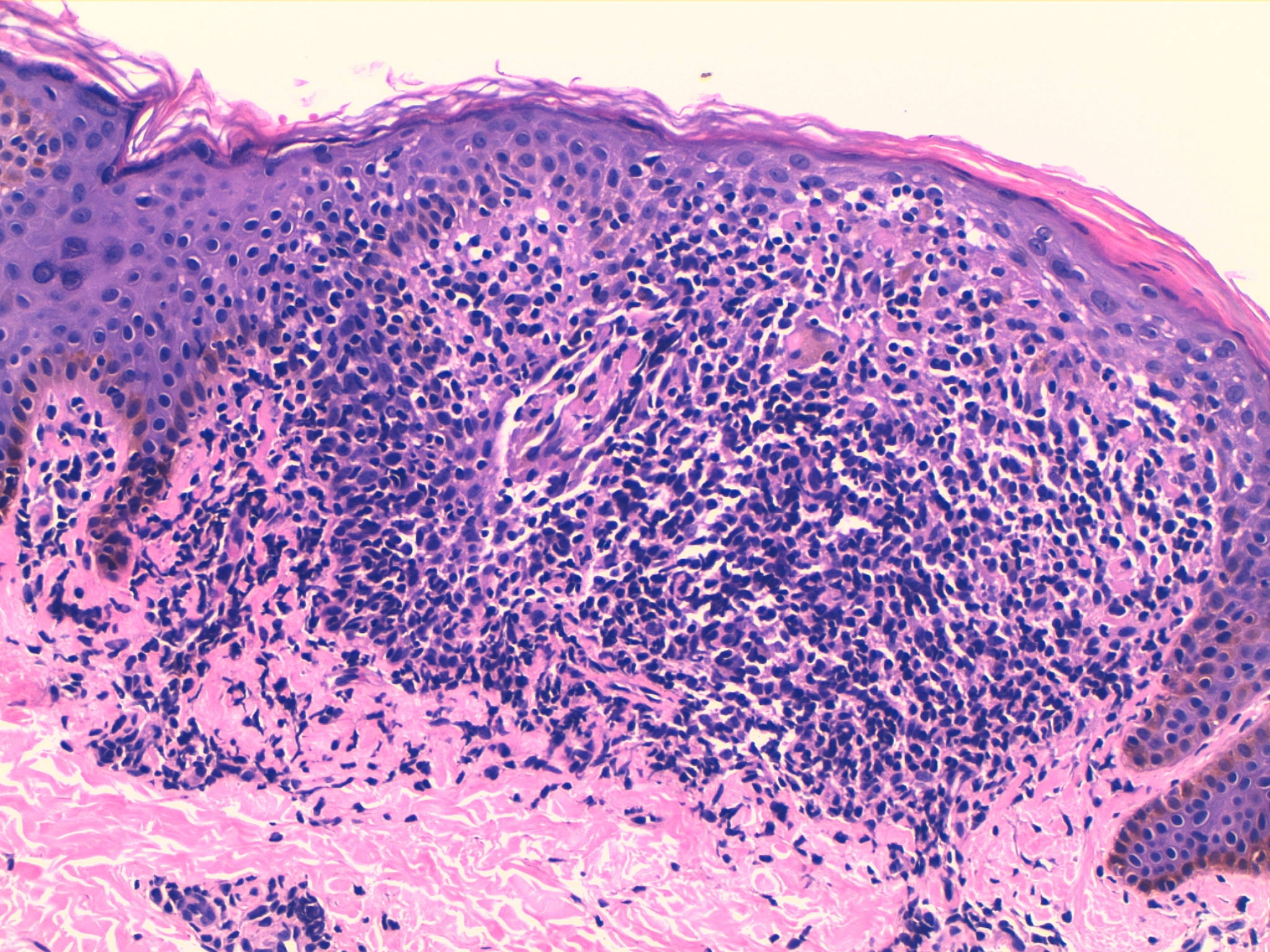
| Figure 3. Well circumscribed inflammatory infiltrate in the epidermis and papillary dermis (H&E x10). Figure 4. Close view-up showed a flattened epidermis and a focal granulomatous inflammatory infiltrate with lymphocytes, histiocytes, and scattered multinucleated giant cells. These were engulfed by elongated rete ridges producing a so-called “claw clutching a ball” pattern (H&E x4). |
|
A healthy 3-year-old boy came to our department for a linear asymptomatic eruption that had been present since birth. He had been unsuccessfully treated with topical steroids. On physical examination, we found numerous tiny whitish flat-topped papules on the anterior trunk with a linear distribution and a few similar lesions on the elbows (Figures 1 and 2). The oral mucosa, palms, soles, and nails were spared. A biopsy was taken from one of the papules on the anterior trunk and the histologic examination demonstrated parakeratosis, a flattened epidermis, and a focal granulomatous inflammatory infiltrate with lymphocytes, histiocytes, and scattered multinucleated giant cells in the epidermis and papillary dermis immediately subjacent to the epidermis. These were engulfed by elongated rete ridges producing a “claw clutching a ball” pattern (Figures 3 and 4). The condition remained unchanged after 6 months of follow-up.
Lichen nitidus (LN), a rare condition of unknown etiology, is characterized by numerous tiny, discrete, skin-colored, uniform, pinhead-sized flat-topped papules. The lesions tend to occur in groups, primarily on the abdomen, chest, glans penis, and/or upper extremities. Generalized forms of LN may be seen occasionally in children [1]. Linear lichen nitidus is very rare [2]. This linear distribution is thought to relate to a Koebner phenomenon. Other unusual clinical variants of LN include confluent, vesicular, hemorrhagic, palmar and plantar, perforating, and familial forms.
The differential diagnosis of LN includes lichen planus (LP), lichen striatus, guttate lichen sclerosus, lichen scrofulosorum, lichen spinulosus, papular sarcoidosis, lichenoid secondary syphilis, frictional lichenoid dermatitis (elbows and knees), papular eczema (especially in skin types V and VI), and flat warts. All of these diseases (except LP) can usually be excluded relatively easily on the basis of clinical and histological findings. The histologic appearance of LN is highly characteristic, showing a downward enlargement of the epidermal rete ridges circumscribing the focal inflammatory infiltrate (“the claw clutching a ball” picture).
The relationship of LN with LP is unclear. Although there are clinical and histologic differences between both entities, there are patients in which LN has progressed to LP. Both diseases can even co-exist and some authors consider LN to be a micropapular variant of LP [3]. However, immunohistochemical studies suggest that these are two different diseases. The cellular infiltrate in LN is heterogeneous, whereas the majority of cells seen in LP are helper T cells. It suggests that the immunologic mechanisms responsible for the diseases are different and probably also explains the different epidermal changes that characterize the two diseases [4].
Because the majority of patients experience spontaneous clearing, treatment is primarily symptomatic. When significant pruritus is present, topical corticosteroids and oral antihistamines may be helpful. Persistent lesions can pose therapeutic challenges. Reported therapies include systemic corticosteroids, levamisole, systemic cetirizine, acitretin, itraconazole, and topical dinitrochlorobenzene [5, 6, 7]. Psoralen and ultraviolet A (PUVA) and narrow band ultraviolet B phototherapy have also been tried with good results [8, 9]. In the majority of cases, especially in infants, a wait-and-see approach is the best option considering the benign course of this disease and frequent spontaneous resolution.
© 2013 Dermatology Online Journal