
|
| Figure 1 |
|---|
| Figure 1. Symmetrical raised brown colored papule of 4 mm in diameter on the right foream of adult female |
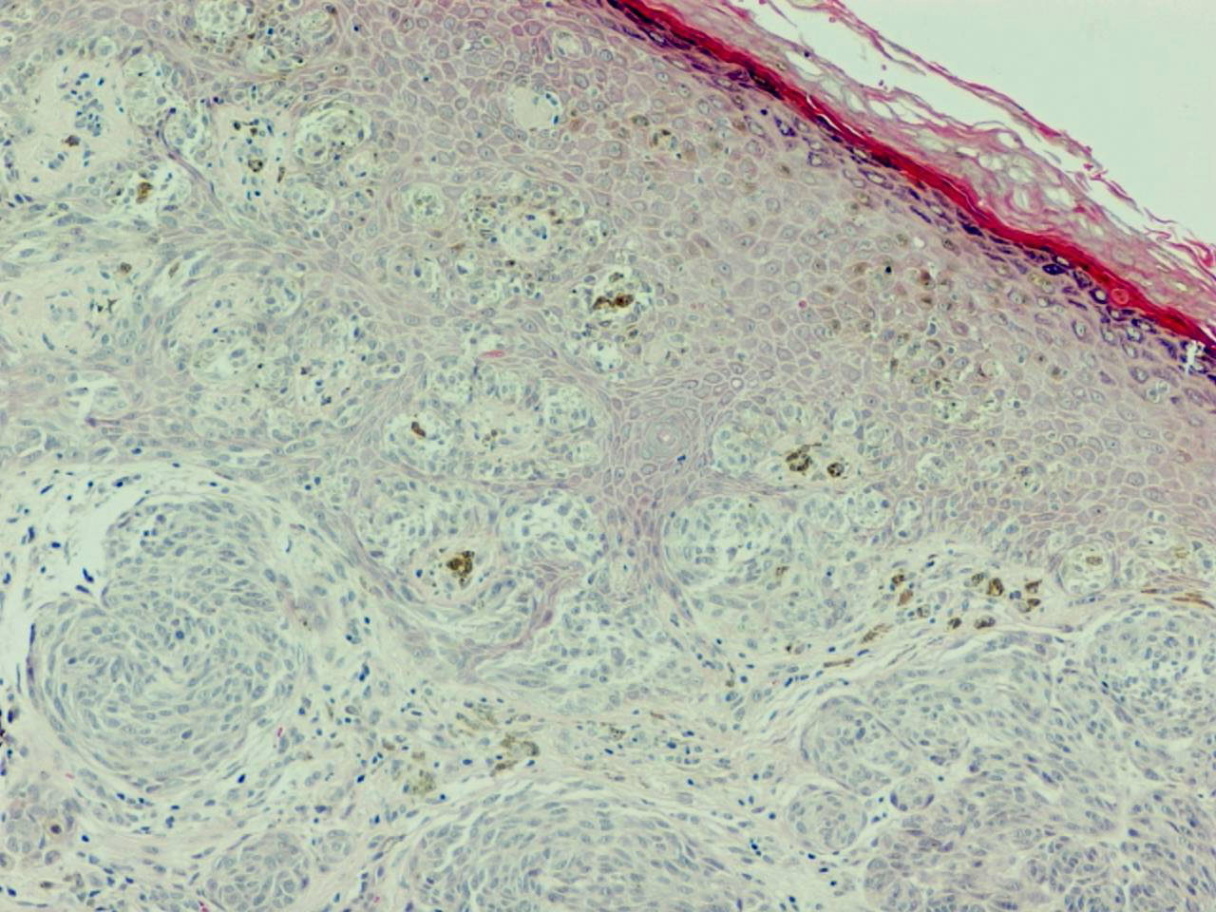
Because of concern for melanoma, a 1 cm margin excision was performed. Histopathological evaluation and immunohistochemical tests including H & E (Figs. 2 - 6), S100 protein (Fig. 7), HMB 45 (Fig. 8), and CD99 (Fig. 9) were performed. In the H & E sections, nests of atypical melanocytic, epitheloid, and spindle cells in the superficial dermis with pagetoid spread in the epidermis were identified (Fig. 2).
 |
 |
| Figure 2 | Figure 3 |
|---|---|
| Figure 2. Nests of non-pigmented spindled melanocytes are present at the dermoepidermal interface and deeper in the dermis with irregular epidermal hyperplasia (H&E, x40). | |
 |
| Figure 4 |
|---|
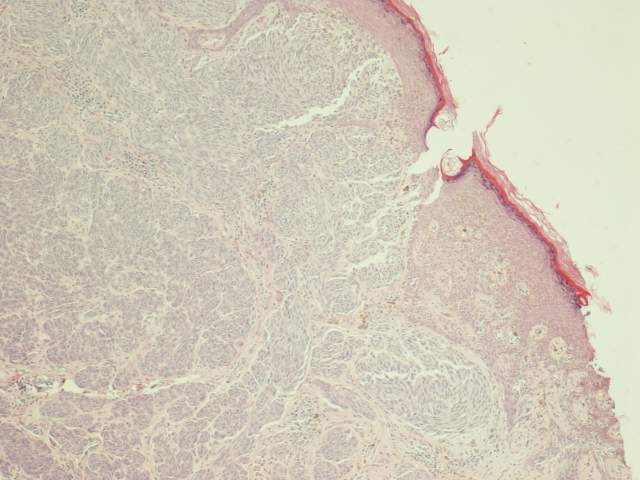
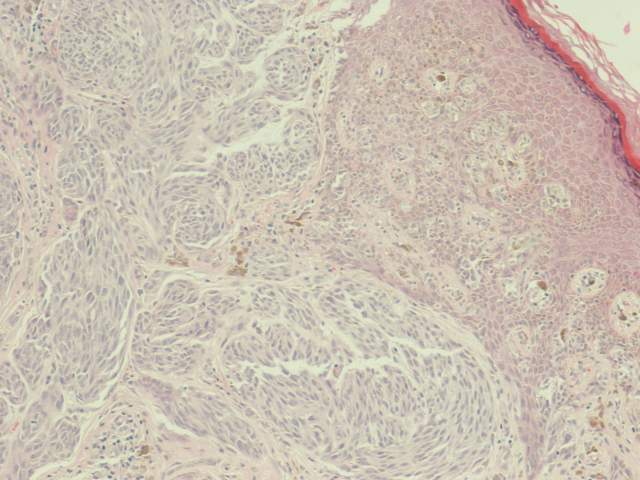
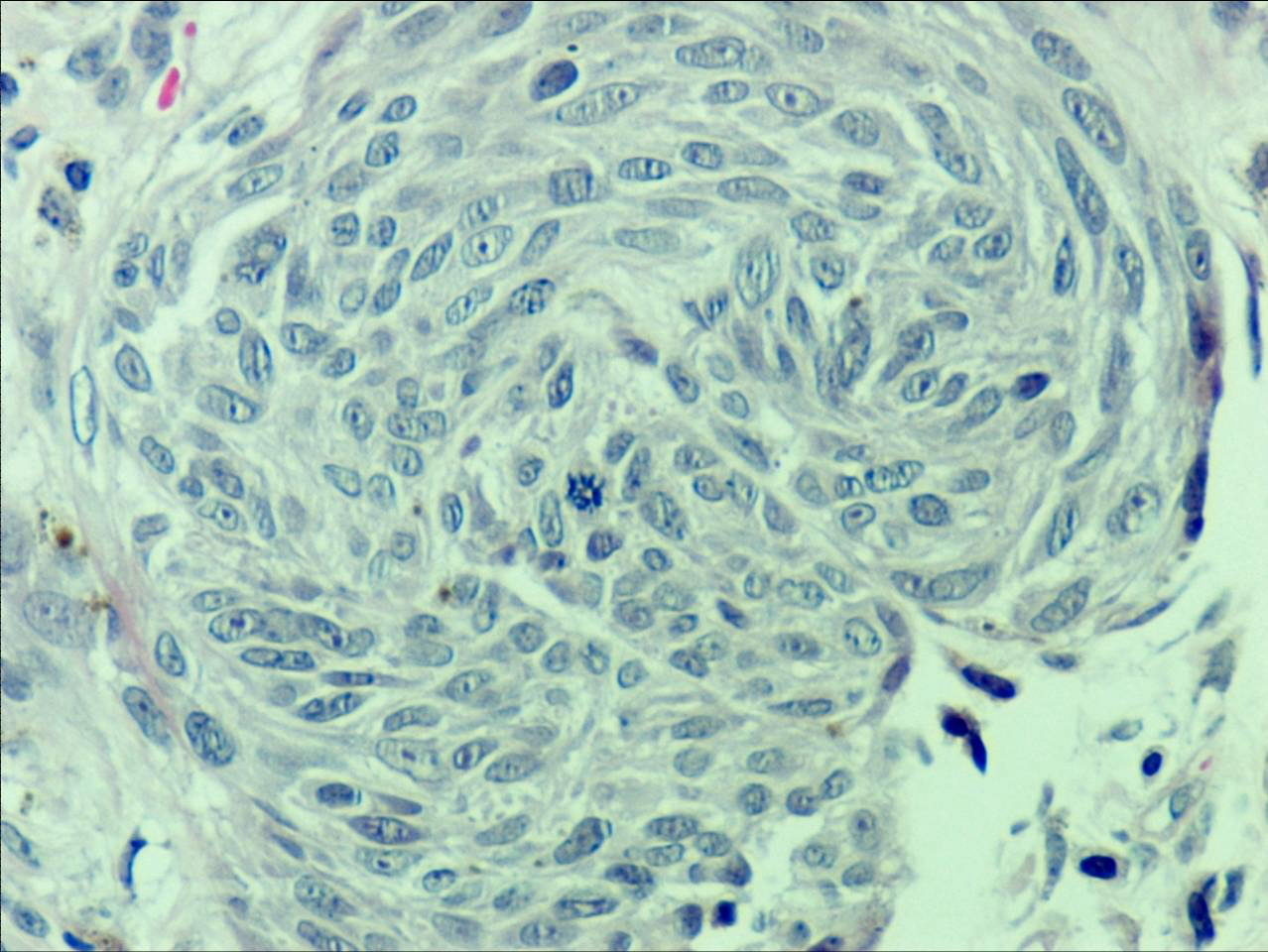
| Figures 2-4. Microscopic views of the lesion with different magnification powers showing nests of the nevus cells. |
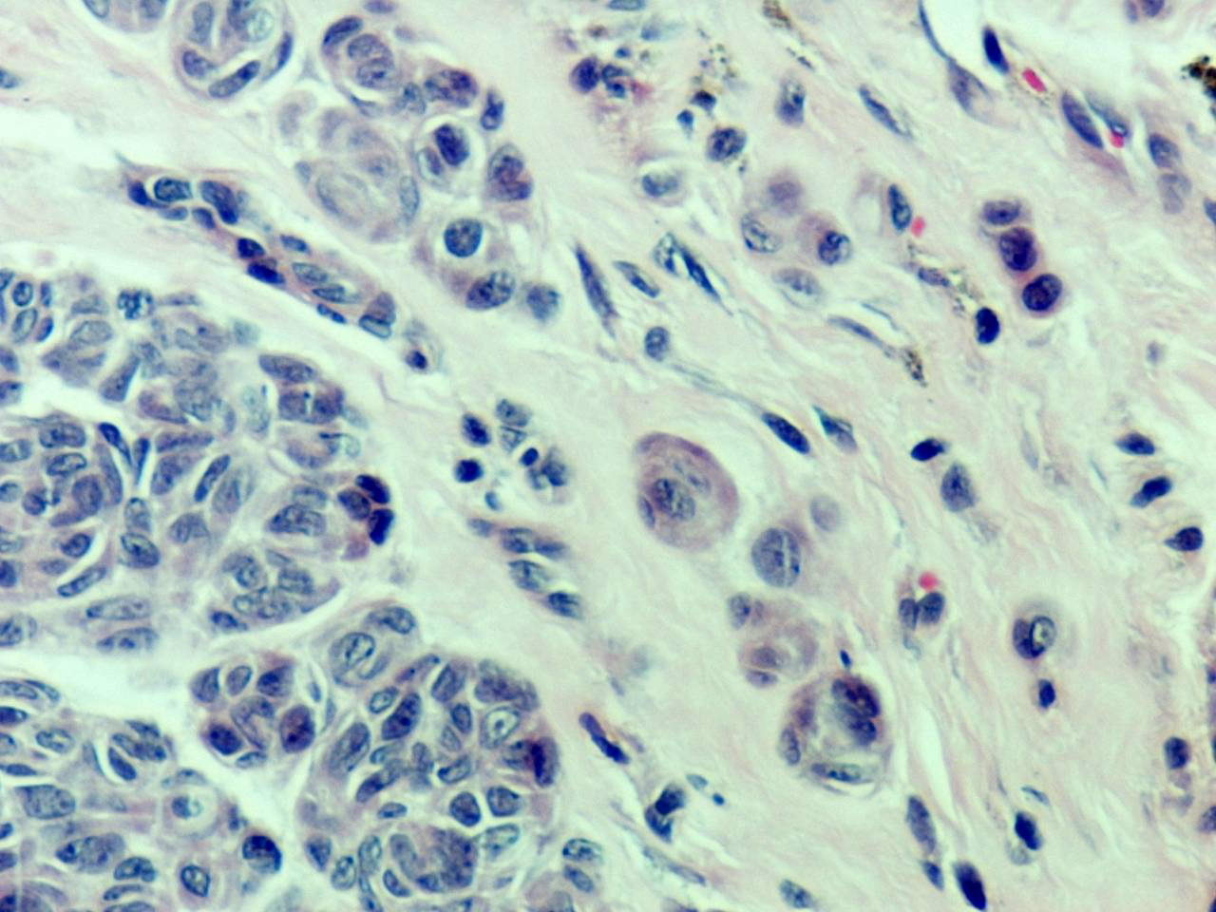
There was focal hypergranulosis and a few Kamino bodies noted. The nevus cells were mainly mononucleated with abundant eosinophilic cytoplasm that exhibited large nuclei with prominent nucleoli. Some were binucleated cells with minimal mitoses. The nests and individual cells were decreasing in size in deeper areas of the dermis.
 |
 |
| Figure 5 | Figure 6 |
|---|---|
| Figure 5. Maturation in the deeper dermal levels where nests contain melanocytes fewer in number and smaller in size Figure 6. Nests of spindle shaped melanocytes in the upper dermis showing occasional mitoses and binucleation. |
|
 |
| Figure 7 |
|---|
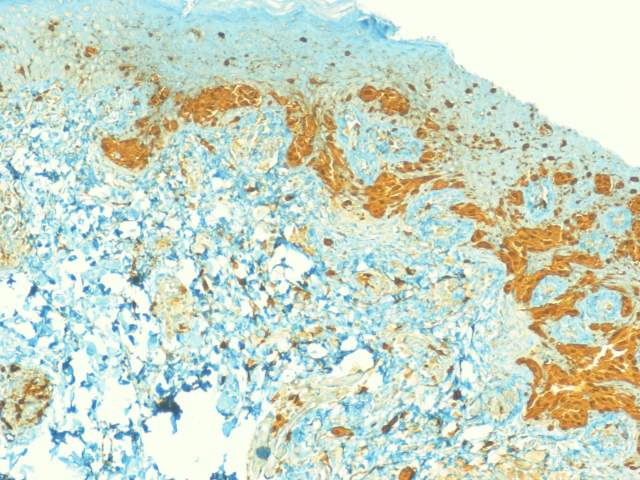
| Figure 7. S100 staining the all the melanocytes with intense staining at the dermal-epidermal junction |
Minimal inflammatory infiltrate was surrounding the lesion. Immunostaining with S100 protein was positive; HMB-45 antigen was minimally positive at the junction.
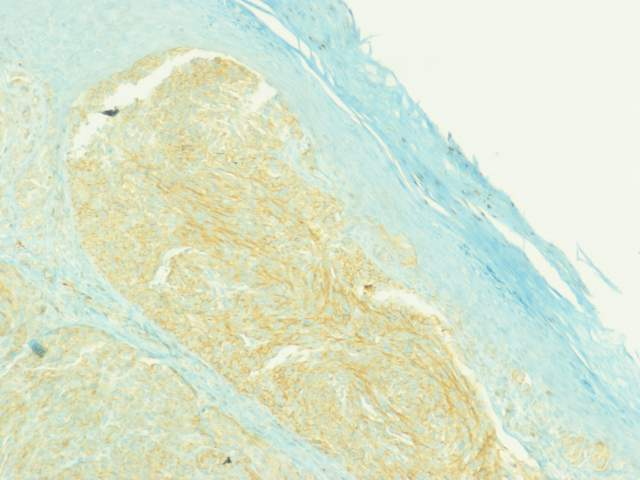
All tumor cells stained with CD99, symmetrically and mainly peripherally in each cell. Therefore, the diagnosis of Spitz nevus was made, but malignant melanoma was not completely ruled out. Follow up of the patient after 3 years did not reveal any recurrence locally or systemically.
 |
 |
| Figure 8 | Figure 9 |
|---|---|
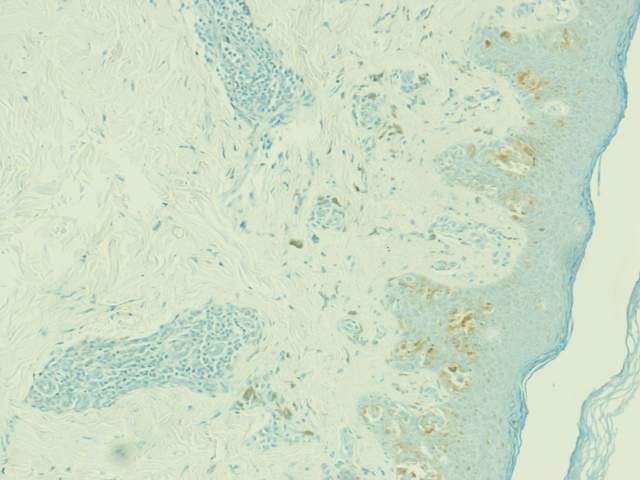
| Figure 8. HMB 45 special staining Figure 9. CD99 special staining |
|
Spitz nevus is a clinico-pathologic entity that can cause diagnostic concern and disagreement among dermatologists and dermatopathologists. In one clinico-pathological study, patients older than 20 years comprised 66 percent of cases, with a predominance of females. The lower extremities were more affected in females, whereas the trunk was more affected in males [1]. Spitz nevus is considered a benign solitary lesion that histologically shows acanthosis, parakeratosis, pagetoid infiltration, and Kamino bodies with multinucleated melanocytes [1]. Genomic DNA studies from Spitz nevi by comparative genomic hybridization (CGH) showed that the majority of Spitz nevi have a normal chromosomal complement at the level of CGH resolution. These findings differ significantly from the previously reported changes in primary cutaneous melanoma and could represent a basis for developing adjunctive techniques for refining accuracy in the difficult differential diagnosis of spitzoid melanocytic neoplasms [2, 3]. In one study, an overwhelming majority of neoplasms that were reported to be "atypical Spitz's nevus," "metastasizing Spitz's nevus," and "malignant Spitz's nevus" were, in fact, melanomas. This further substantiates the diagnostic difficulties posed by many Spitz tumors, especially those with atypical features. Observations do suggest that a biological relationship exists between the Spitz nevus and malignant melanoma [4, 5]. Immunohistochemical studies have shown that 56 percent of melanoma and only 5 percent of Spitz nevus express CD99. However, this does not elucidate the role that CD99 plays in these melanocytic processes. It does show that CD99 may be a useful tool in distinguishing malignant melanoma from Spitz nevus [6]. In general, to differentiate Spitz nevus from malignant melanoma, the patient's age provides a critical piece of clinical information. Spitz nevi occur mostly in children and melanomas occur mostly in adults. Nevertheless, there is overlap in the age distributions of Spitz nevus and melanoma. In addition, the following histological features should make one question a benign diagnosis: cells with abundant pale or dusty cytoplasmic melanin pigmentation pattern, cells with very large eosinophilic nucleoli, and cells with uniformly hyperchromatic nuclei [7]. Malignant melanoma was an important concern in this patient. Although she has had no recurrences after 3 years of follow up, we continue to monitor her. There is controversy regarding adequate treatment for a Spitz nevus due to concerns about the accuracy of the diagnosis. Therefore, it is usually recommended that Spitz nevi be completely excised and some recommend a 5mm margin [8, 9]. In conclusion, Spitz nevus can be difficult to diagnose in some cases with atypical presentation. Until definite and specific criteria are developed for the diagnosis of Spitz nevus, malignant melanoma should be in the differential.
© 2009 Dermatology Online Journal