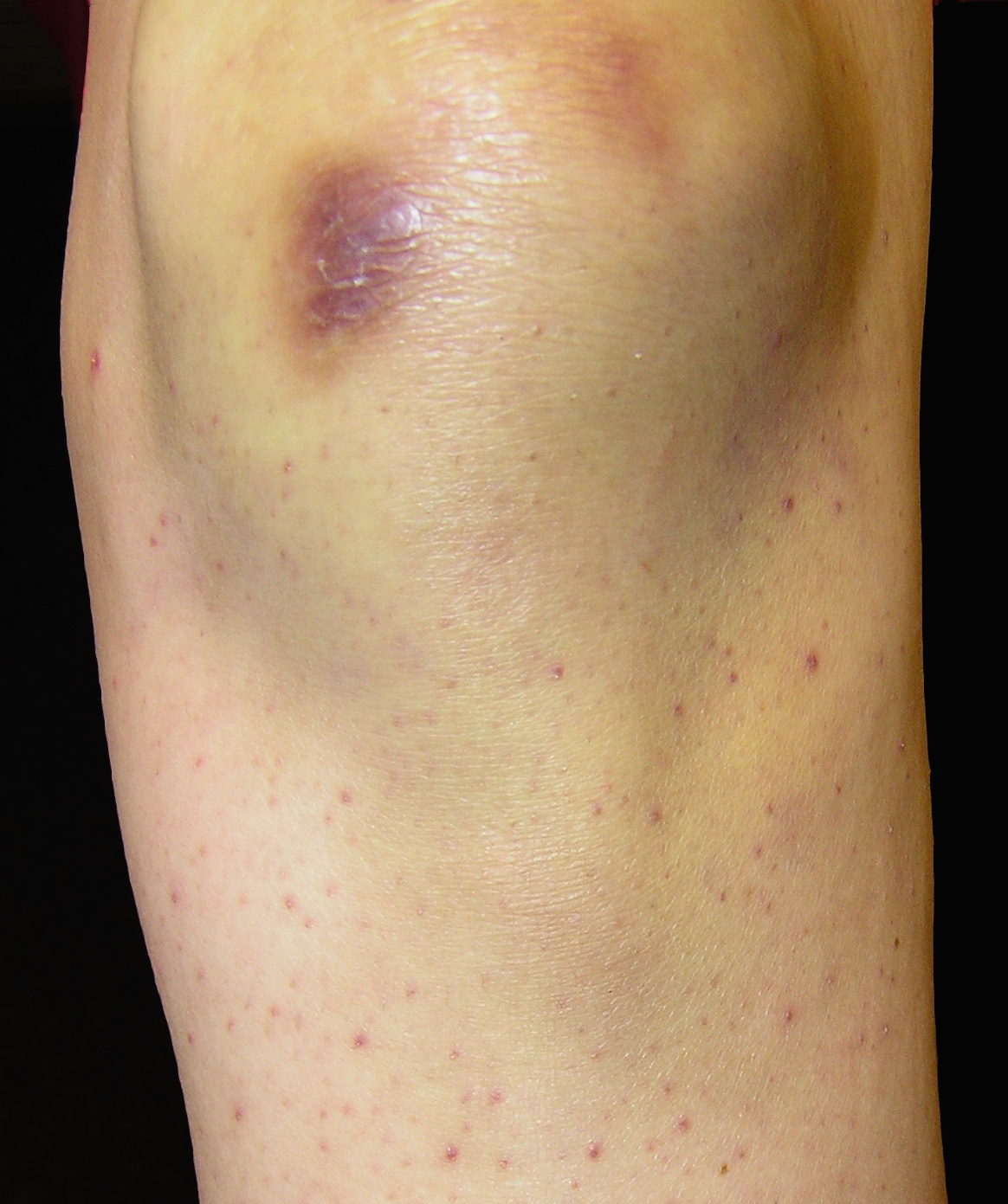

Figure 2. Close-up image.
The patient was on a self-imposed, limited diet with essentially no citrus fruit products. A serum vitamin C level was undetectable at <0.12 mg/dL, confirming a diagnosis of scurvy. Vitamin C supplementation (500 mg daily) was initiated and occurred complete resolution of the skin lesions over the next few weeks.
|
|
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Purple papules on the leg. Figure 2. Close-up image. |
|
Although scurvy is primarily thought of as a disease of sea voyagers, it was first described in writings from as far back as 1500 BC [5]. It led to the demise of many individuals before Sir James Lind, a navy surgeon documented that citrus fruit consumption could prevent and treat scurvy [5]. It was not until 1931 that Albert Szent-Gyorgyi identified the active substance in fruits and vegetables—ascorbic acid, now known as vitamin C [5]. Despite being considered a disease of the past when diets, particularly those of some sailors, were limited in citrus fruits, several recent articles have reported cases in the United States and other industrialized nations [1, 4, 5]. A study by Olmedo and colleagues identified many at risk groups including: food faddists, patients with colitis, chemotherapy patients, widowers, those suffering from anorexia nervosa, individuals with major depression disorder, and schizophrenics [5]. In another study, additional risk factors associated with scurvy included alcohol abuse and tobacco abuse [2].
Humans are one of the few animals that cannot synthesize vitamin C, so our total body pool is dependent on dietary intake and intestinal absorption [4]. This nutrient is absorbed by active transport in the ileum [2]. Approximately 85 percent of the ingested vitamin is absorbed, but the transport mechanism can become saturated. Therefore, divided doses are preferred [2]. In healthy individuals, the kidneys can reabsorb ascorbic acid, but it is lost during hemodialysis [5]. The recommended dietary allowance for vitamin C was recently increased by the Food and Drug Administration (75 mg daily for females, and 90 mg daily for males) [5]. However, pregnant and lactating women, smokers, and alcoholics require more vitamin C [3]. Clinical manifestations of scurvy appear when the total body pool is less than 350 mg [5]. This occurs after a diet free of vitamin C for 60 to 90 days and is prevented by daily intake of just 10 mg [1, 5].
Scurvy is a disease that affects multiple organ systems because the functions of vitamin C are so diverse. Ascorbic acid is a cofactor for protocollagen proline hydroxylase [1]. If not present, there is under- hydroxylation of protocollagen and defective assembly of mature collagen triple helices [1]. The defective collagen leads to impaired synthesis of basal lamina, media, and adventitia of blood vessels and results in a hemorrhagic diathesis and poor wound healing [3].
Vitamin C is also involved in the metabolism of tyrosine and the synthesis of catecholamines [2, 5]. In addition to its antioxidant properties, it aids iron absorption from the small intestine and is required for the disulfide bonding of hair [5]. It is the combination of defects in these processes that lead to the clinical manifestations of scurvy.
The first symptoms are nonspecific, including fatigue, weakness, myalgias, diarrhea, and depression [1, 3]. The initial dermatologic signs are follicular hyperkeratoses and coiled corkscrew hairs [1]. Blood vessel fragility resulting from impaired collagen synthesis results in perifollicular hemorrhages, petechiae, and ecchymoses [1]. Broken hairs are due to abnormal disulfide bonding and keratin formation [4]. Other signs include nail splinter hemorrhages and occasionally alopecia [4]. In 80 percent of cases, musculoskeletal manifestations and oral cavity changes are also identified [2, 5]. If the vitamin C deficiency continues undetected, seizures and cardiac abnormalities may occur - sudden death has even been reported [2]. The mechanism of the cardiac dysfunction is unclear, but is hypothesized to be secondary to impaired vasoconstriction to adrenergic stimuli causing syncope, refractory hypotension, and high output heart failure [3, 5].
Scurvy is primarily a clinical diagnosis; skin biopsies are usually nonspecific and lab testing is often unnecessary [1, 5]. Because the vitamin C levels are greatly affected by recent dietary intake, normal or increased levels do not rule out the diagnosis, but a low level of serum ascorbic acid is diagnostic [1]. Treatment with vitamin C replacement results in rapid resolution of most of the manifestations [3].
Scurvy is not a disease of the past. It is a disease that requires physicians to maintain a high index of suspicion to recognize the many clinical manifestations. Although it is a multi-system disease, often the initial diagnosis is based on cutaneous signs and symptoms [1]. Early recognition and treatment is essential to prevent the serious consequences of long-term vitamin C deficiency.
© 2008 Dermatology Online Journal