Angiolymphoid hyperplasia with eosinophilia
Published Web Location
https://doi.org/10.5070/D36613z8tnMain Content
Angiolymphoid hyperplasia with eosinophilia
Arash K. Asadi
Dermatology Online Journal 8(2): 10
From New York University Department of DermatologyHistory
The patient is a healthy 43 woman with a 20-year history of pruritic lesions on her ears and periauricular areas. The lesions started insidiously with no tendency for spontaneous resolution. Previously, she had been treated with excisions, liquid nitrogen cryotherapy, electrodesiccation, and intralesional glucocorticoids, all of which provided temporary improvement but no lasting benefits. Moreover, the use of 585-nm, pulsed-dye laser treatment to several lesions was associated with resolution with recurrence after one month. Most recently, she underwent 12 sessions of radiation therapy, which led to a remission that lasted approximately six months. Since her most recent recurrence, she has been using topical medium-potency glucocorticoids, doxepin cream, and topical anesthetics to achieve variable and brief symptomatic improvement.
Physical Examination
 |  |
| Figure 1 | Figure 2 |
|---|
Approximately eight, 2-mm, dome-shaped, erythematous papules were present on the helices, triangular fossae, conchae, and posterior surfaces of both ears as well as on the postauricular areas. Occasional excoriations were noted.
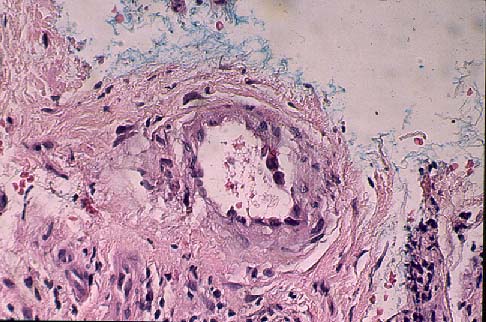
Histopathology
There is a proliferation of thick-walled blood vessels which are lined by prominent endothelial cells, some of which have cytoplasmic vacuoles. There is a dense, perivascular and interstitial infiltrate of lymphocytes, plasma cells, and eosinophils.
Comment
Angiolymphoid hyperplasia with eosinophilia primarily affects middle-aged Caucasian women with persistent and recurrent erythematosus or hyperpigmented, dome-shaped, dermal papules or nodules of the head and neck. Although there is a predilection for the periauricular area, involvement of other skin surfaces as well as the oral mucous membranes, pharynx, and orbit has been reported. The lesions, which are often pruritic or painful, may coalesce into confluent plaques that are chronic with little propensity for spontaneous resolution. In some cases, peripheral blood eosinophilia is present. Systemic spread has not been reported.
Histologically, there is both a vascular and an inflammatory component. There is a proliferation of small-sized blood vessels lined by enlarged endothelial cells as well as aggregates of non-canalized, plump endothelial cells. There is a perivascular inflammatory infiltrate composed of lymphocytes as well as eosinophils and mast cells. Although the literature tends to favor a reactive process, there is some debate as to whether angiolymphoid hyperplasia with eosinophilia is a reactive or neoplastic disease.
There is no consistently effective treatment for this disease. Intralesional injections of glucocorticoids, interferon alpha-2a, and cytotoxic agents may be effective. Although surgical excision can be curative, recurrences are common. Destructive techniques such as cryotherapy and electrodesiccation may be attempted. In addition, pulsed-dye lasers have been used to selectively target the vasculoproliferative component of this disorder. Multiple laser treatments are generally necessary to cause resolution of the lesions. The use of a long-pulse turntable dye laser has been advocated based on its deeper penetration and greater epidermal sparing properties.
Angiolymphoid hyperplasia with eosinophilia should be distinguished from Kimura's disease, which presents as large, deep, subcutaneous plaques in the periauricular and submandibular regions of young Asian men. Regional lymphadenopathy, peripheral blood eosinophilia, and elevated serum IgE levels are often present. Histologic features of Kimura's disease include prominent lymphoid follicles and fibrosis with a less prominent capillary proliferation and without aggregates of non-canalized endothelial cells.
References
Kung ITM, et al. Kimura's disease: a clinicipathological study of 21 cases and its distinction from angiolymphoid hyperplasia with eosinophilia. Pathology 16:39, 1984Olsen TG, et al. Angiolymphoid hyperplasia with eosinophilia. J Am Acad Dermatol 12:781, 1985
Chun SI, et al. Kimura's disease and angiolymphoid hyperplasia with eosinophilia. J Am Acad Dermatol 27:954, 1992
Rohrer TE, et al. Angiolymphoid hyperplasia with eosinophilia successfully treated with a long-pulsed turntable dye laser. Dermatol Surg 26:211, 2000.
© 2002 Dermatology Online Journal