Mid-dermal Elastolysis
Published Web Location
https://doi.org/10.5070/D37hw4n8s0Main Content
Mid-dermal Elastolysis
Jeremy E. Rothfleisch,MD
Dermatology Online Journal 7(1): 15
Department of Dermatology, New York UniversityPATIENT: 41-year-old man
DURATION: Several months
DISTRIBUTION: Abdomen and lower back
History
The patient presented to the New York Harbor Health Care System Dermatology Clinic with a two to three month history of asymptomatic papules on his abdomen and lower back. His past medical history and review of symptoms were noncontributory. There has been no treatment.
Physical examination
Multiple, discrete, wrinkled, flesh-colored, soft papules, some with a central umbilication, were present on the abdomen and lower back. There was no scale. Darier's sign was absent.
 |  |
| Figure 1 | Figure 2 |
|---|
Laboratory data
None
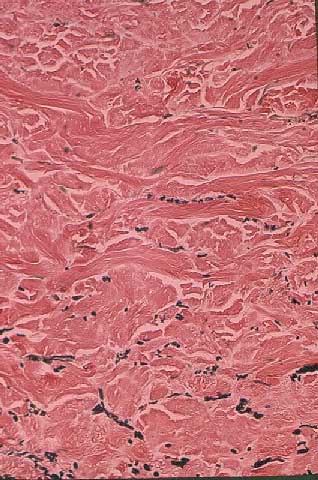
Histopathology
There was selective absence of elastic fibers in the mid-dermis as detected with the Verhoeff-van Gieson stain.
Diagnosis
Mid-dermal elastolysis
Comment
First described by Shelley and Wood in 1977, mid-dermal elastolysis is an idiopathic condition which exhibits loss of mid-dermal elastic tissue.[1,2,3] Clinically, two morphologic patterns are noted: small wrinkles arranged parallel to the skin cleavage lines (type 1) and very small, soft, papular lesions composed of perifollicular protrusions, which leave an indented center at the follicular orifice (type II).[4] Although the patient presented represents type II mid-dermal elastolysis, there is also a loss of papillary dermal elastic fibers, and he may be categorized as an overlap form with upper dermal elastolysis.
Upper dermal elastolysis differs from mid-dermal elastolysis not only in the location of the absent elastic fibers but also in the severity of ultrastructural damage.[4] Both conditions consist of irregularly branched or lumpy elastic fibers, in which the assembly of component fibrils is loose and electron-dense substances are aggregated in the spaces between these loosely bound subunit fibrils and along the periphery of abnormal fibers. It has been suggested that both conditions may be the result of elastophagocytosis by dermal macrophages. Electron microscopy also has shown that neither condition involves other constituents of the dermis, such as collagen fibers, vessels, or fibroblasts.
Mid-dermal elastolysis most likely represents a post-inflammatory elastolysis inasmuch as lesions have been associated with urticaria, solar urticaria, and granuloma annulare.[5] Another hypothesis is that lesions not believed to be preceded by another dermatoses may represent unknown types of inflammatory elastolysis, which were clinically asymptomatic but sufficient in intensity to cause destruction and disappearance of elastic fibers.
There is no currently known treatment for this condition, but some have proposed the use of retinoids or colchicine. Oral and topical glucocorticoids are known to be ineffective.
References
1.Shelley WB, Wood MG. Wrinkles due to idiopathic loss of mid-dermal elastic tissue. Br J Dermatol 1977;97(4):441-5. PubMed2.Rudolph RI. Mid dermal elastolysis J Am Acad Dermatol 1990;22(2pt1):203-6. PubMed
3. Sterling JC, Coleman N, Pye RJ. Mid-dermal elastolysis [see comments] Br J Dermatol 1994;130(4):502-6. PubMed
4. Hashimoto K, Tye MJ. Upper dermal elastolysis: a comparative study with mid-dermal elastolysis. J Cutan Pathol 1994;21(6):533-40. PubMed
5. Yen A, Tschen J, Raimer SS. Mid-dermal elastolysis in an adolescent subsequent to lesions resembling granuloma annulare. J Am Acad Dermatol 1997;37(5 Pt 2):870-2. PubMed
© 2001 Dermatology Online Journal