Ultraviolet light is an environmental factor aggravating facial lesions of adult atopic dermatitis.
Published Web Location
https://doi.org/10.5070/D30jk73412Main Content
Ultraviolet light is an environmental factor aggravating facial lesions of adult atopic dermatitis.
H. Deguchi, N. Umemoto, H. Sugiura, K. Danno and M. Uehara
Dermatology Online Journal 4(1): 10
An increasing number of adult patients with atopic dermatitis (AD) in Japan are distressed by persistent eczematous lesions of the face (so-called atopic red face) (Fig. 1). Phototests were carried out in 28 patients with the atopic red face to test a possibility that ultraviolet (UV) light could be an aggravating factor. Contact and photocontact dermatitis had been ruled out by repeated patch and photopatch tests. All of the patients had a normal response to a screening dose of UVA (10 J/sq cm) and a normal minimal erythema dose (MED) of UVB. Ten of these patients, however, showed an abnormal papular response to a single or 3-times consecutive UVB radiation above the MED (90 mJ/sq cm) (Fig. 2). |


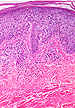
Histological examination of the UVB-induced papular lesions, performed in 3 patients, showed epidermal spongiosis and lymphocytic infiltration in the upper dermis and epidermis (Fig. 3). Immunohistochemically, CD4+ infiltrating cells (Fig. 4) were dominant to CD8+ cells (Fig. 5) (ratio, 6.1 - 8.6) , and many of them were positive for OKT 6. |
 |  |
| Figure 4 | Figure 5 |
|---|---|
The findings favor the provocation of AD lesion itself by UVB rather than a polymorphous light eruption that may coexist with AD because a CD4/CD8 ratio in the latter condition is reportedly as low as 1.0. The results of the phototests suggest that UV light may be one of the aggravating factors of the atopic red face.
Discussions

J Epstein: This is a most interesting report. One of the more difficult issues in photomedicine for me has been differentiating between patients with photoaggravated atopic dermatitis and those with polymorphous light eruption (PMLE) and atopic dermatitis. Since both PMLE and atopic dermatitis are relatively common diseases, their occurrence in the same patient would not be unexpected. Perhaps, the CD4+ to CD8+ ratio in the infiltrate as Deguchi and coworkers have pointed out will provide such a marker.
What is your opinion?

K Danno: Abnormal, papular UVB reactions as we have shown in some of adult atopic dermatitis patients with persistent, eczematous lesions of the face (so-called red face) may suggest photoaggravating atopic dermatitis or the co-existence of a polymorphous light eruption. Agreeing with Dr. John Epstein's comments, these two conditions are hardly differentiated based on the results of the UVB tests alone. However, the clinical features of the patients after sunlight exposure were the exacerbation of the red face itself, and no lesions suggestive of PLE were induced in other part of the body including face and hand dorsa. The high CD4/CD8 ratio among the infiltrated lymphocytes of the UVB test sites was more like the acute eczematous lesions of atopic dermatitis than PLE, but the difference of the immunopathological characteristics may alternatively depend on the stage of the diseases.

J Hanaffin: The report by the Shiga group is of considerable interest, both because of the serious problems associated with the *atopic red face* and the longstanding uncertainty associated with atopic photosensitivity. The latter was studied by Frain-Bell many years ago (Br J Dermatol 85:105, 1971), but no consistent findings have ever been demonstrated.
KD: Although much attention has been paid to the atopic red face of the Japanese adult patients, causes are still unknown. Multiple exacerbating factors, such as corticosteroids and environmental influences, may be related to this severe, intolerable symptom. Dr. Frain-Bell has suggested that photosensitivity is associated with atopic dermatitis at least in a few infants. In this study, we have carried out standard light tests in a large group of the subjects and found that more patients beyond expectation had photosensitivity to UVB.
JMH: In the present study, about one-third of 28 patients with atopic red face developed papular lesions after one to three exposures of UVB at 90 mJ/sq cm. These were said to be slightly above the MED. The normal MED in Japan is listed as 50 - 150 mJ (Imamura handbook), so it is unclear whether some of these patients had generally reduced MED thresholds. It would be helpful to know the ratio of the 90 mJ UVB dose to their individual MED*s. Patients had been screened with patch and photopatch tests, tending against photocontact allergy. UVA phototoxicity also appears unlikely.
KD: The minimal erythema dose (MED) of UVB was normal in all of the examined cases except one in which the MED was markedly decreased. Three consecutive irradiation of UVB light at the dose equivalent to one or 1.5 MEDs induced an abnormal, papular response at the test site (lower back). Our previous study has demonstrated that only three of 120 patients with severe atopic dermatitis showed UVA photosensitivity. One of them was found to be antihistamine- induced.
JMH: The authors suggest these reactions are exacerbations of AD, and that has long been an assumption for the much milder atopic photosensitivity we see in most parts of the United States. This condition may be more evident in the Los Angeles area (personal communication, M. Rappaport, 1997). If confirmed, this would further support a UV association. I am concerned, however, that there may be a genetic influence as well as an environmental influence acting to create the red face syndrome. The possibility of polymorphous light eruptions (PMLE) remains, possibly analogous to the striking PMLE prevalence in some groups of American Indians. More studies are needed in which phototesting and biopsies from red face patients are compared with PMLE controls. Even then, PMLE histology may be atypical in patients with AD. Unfortunately, cell markers are not yet specific enough to allow firm distinctions.
KD: In all of the light test-positive patients, exacerbation of the facial lesions did not decay within one day but persisted longer than a few days, suggesting that the results of the light tests are well correlated with their clinical conditions. However, UVB photosensitivity in red face patients was hardly differentiated from PMLE controls. It is also possible that influences other than UV light may contribute to the exacerbation of the red face.
JMH: These preliminary studies are most interesting and point up the need for further investigation of the UV role in red face
AD.
© 1998 Dermatology Online Journal