Painful leg lesions: A Case Report
Published Web Location
https://doi.org/10.5070/D38rg7v60gMain Content
Painful leg lesions: A case report
Edward Zabawski, Jr., D.O., Laura Dollison, D.O., and Alan Rudick, D.O.
Dermatology Online Journal: 3(1): 4
AbstractWe describe a case of Löfgren's syndrome where the characteristic history and physical exam allowed for the provisional diagnosis to be made in the emergency department. The diagnosis was subsequently confirmed by hilar lymph node biopsy demonstrating noncaseating granulomas. The prognosis and treatment are briefly reviewed. |
Introduction26 year old white male presented to the Emergency Department with a 5 day history of "painful bruises" that began as a solitary area on the right lower extremity. He stated that he had come to the hospital because these areas were becoming more painful, more numerous, and seemed to be occurring more proximally on both of his legs. None of these lesions had occurred above the knee and no erosion or ulceration had developed. The patient also complained of peculiar joint pain in the fingers, wrists, ankles, knees and toes. The arthralgias began about the same time as the "bruises" and were aggravated by joint motion. Review of systems was significant for a dry cough, malaise, and decreased appetite over the same 5 day period. Except for low back surgery about a month earlier, he reported having been in good health. The patient stated he had not traveled outside of his home state (Ohio) since 1991 and had never worked in a factory, foundry, farming operation, mental health facility or nursing home. He reported that he owned no pets and did not use alcohol, tobacco or illegal drugs. Examination of the skin revealed lesions confined to the anterior and medial aspects of both legs. There were multiple erythematous to violaceous swellings (areas of tumescence) which were tender to palpation and warm to touch. The borders were indistinct, some lesions were discrete while others appeared to coalesce. Diascopy was attempted but the exam was limited by the tenderness. The right leg was more involved than the left. No erosions, ulcerations or edema was noted. The remainder of the clinical exam was unremarkable. No swelling, tenderness, erythema or restriction of motion of any of the joints could be appreciated. |

|
| FIGURE 1 | FIGURE 2 |
|---|
|
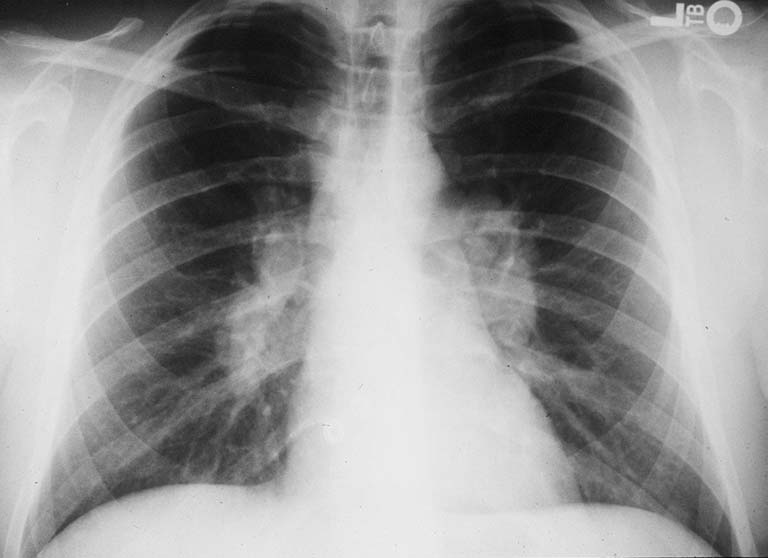
Figure 1: Chest radiograph performed 6 weeks prior to admission. Figure 2: Chest radiograph from the day of admission. Note the development of significant hilar adenopathy. |


|
| FIGURE 3 | FIGURE 4 |
|---|
| Figures 3 and 4: Darkly erythematous to violaceous swellings of the legs |
|
Laboratory examination revealed a normal complete blood count. C-reactive protein level was 9.41 (normal:less than 1 mg/dl) and the ESR was 69. An automated serum chemistry was largely unremarkable, as was the urinalysis. An AP and lateral chest x-ray was obtained an compared with an identical study performed 7 weeks earlier (see Figs 1 and 2). Marked bilateral hilar adenopathy was evident, as were faint peripheral superior and inferior infiltrates. The patient was admitted with a provisional diagnosis and further work-up was obtained. A skin test for tuberculosis was negative, as were serum antibodies for histoplasmosis, blastomycosis, and coccidiomycosis. Sputum culture for acid-fast bacilli showed no growth. A transbronchial biopsy was performed but was histologically nondiagnostic. A biopsy of the hilar lymph nodes via mediastinoscopy was performed which revealed circumscribed epithelioid granulomas with little or no central necrosis. Stains for fungi and acid-fast bacilli were negative. |
|
| FIGURE 5 | FIGURE 6 |
|---|
|
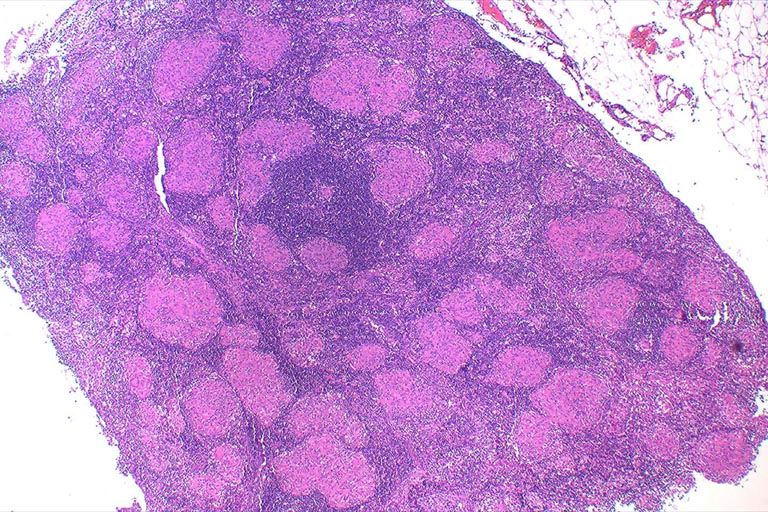
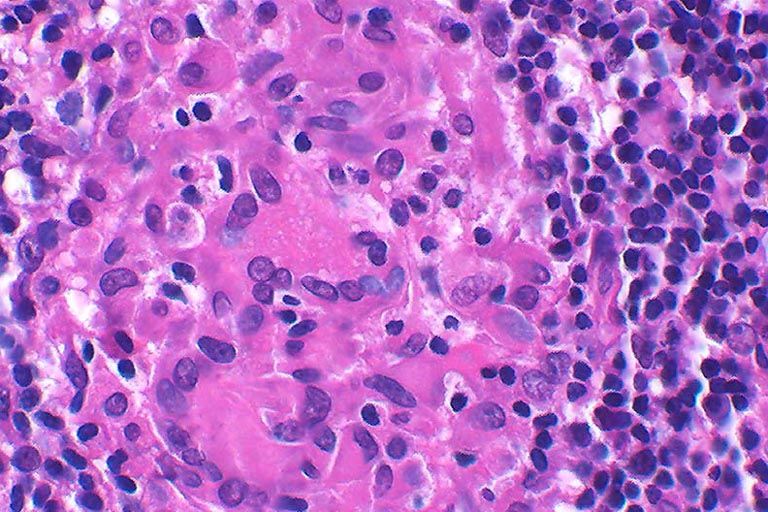
Figure 5: Histopathology of mediastinal lymph node. (original magnification with a 4X objective) Figure 6: High power view of mediastinal lymph node demonstrating giant cells and the absence of caseation. (original magnification with 40X objective)
|
Diagnosis: Löfgren's Syndrome Clinical courseThe patient was admitted with the provisional diagnosis of Löfgren's syndrome. He was initially prescribed a course on non-steroidal antiinflammatory therapy. As in all cases of hilar adenopathy and erythema nodosum, steroids were withheld until infectious or cancerous causes could be excluded. Once the diagnosis of sarcoidosis was confirmed on biopsy and because the patient was not getting satisfactory relief with nonsteroidal antiinflammatory therapy, a course of prednisone was initiated which resulted in significant relief of joint symptoms and skin pain and progression towards clearing of the skin lesions. The patient was subsequently weaned from the prednisone and continues to be free free of skin lesions and joint pain after 11 months of follow up.DiscussionSarcoidosis presenting as the acute onset of erythema nodosum, arthralgia, and bilateral hilar adenopathy was first described by Löfgren in 1952(1). It remains a diagnosis of exclusion. Erythema nodosum with characteristic histopathologic findings of sarcoidosis and elimination of other causes, and bilateral hilar adenopathy are necessary for definitive diagnosis.(2)(3)(6)Löfgren's syndrome occurs most commonly in patients about 30 years of age and is more common in females than males.(2)(4)(5)(7) The occurrence of erythema nodosum was noted by Löfgren to be a positive prognostic sign.(8) Subsequent studies have verified that the presence of erythema nodosum at the time of presentation is the best indicator of a good prognosis in acute sarcoidosis.(4)(5) In a study investigating prognostic factors in sarcoidosis, remission of in patients presenting with arthralgias, erythema nodosum and bilateral hilar adenopathy was noted in 83 per cent of patients at 2 years from diagnosis.(4) Erythema nodosum is usually mild and self-limiting in sarcoidosis, and recurrences are rare.(9)(13) Histologically, the characteristic appearance of sarcoidosis is the presence of circumscribed epithelioid cell granulomas with little or no necrosis and mild or moderate admixture of lymphoid cells at the periphery.(10) The treatment of Löfgren's syndrome depends on the course and severity of the symptoms in individual cases.(13) Non-steroidal antiinflammatory agents (NSAIDs) are usually effective for symptomatic relief, but corticosteroid therapy may be required when NSAIDs are not sufficient.(11) Erythema nodosum should not be treated with corticosteroids until an infectious etiology has been excluded.(12) The immediate availability of laboratory and x-ray services in the emergency department makes it an ideal clinical setting for the evaluation of a patient presenting with with possible Löfgren's syndrome. Acute sarcoidosis may present in an urgent care setting such as an emergency department with the onset of symptoms of short duration( i.e 4-5 days) as it did in this case. The availability of a chest x-ray and screening chemistry profile in that setting make it easier for the physician to make a presumptive diagnosis of Löfgren's syndrome in the patient presenting with erythema nodosum. References1. Löfgren S, Lundback H: The bilateral hilar lymphoma syndrome. Acta Med Scand 1952 ;142:259-273. 2. Winterbauer RH, Belic N, Moores KG: A Clinical Interpretation of Bilateral Hilar Adenopathy. Annals of Int Med 1973;78:65-71 3. Chestnut AN: Enigmas in Sarcoidosis. West J Med 1995; 162:519-526. 4. Neville E, et al.: Prognostic Factors Predicting the Outcome of Sarcoidosis: An analysis of 818 Patients. Quarterly Journal of Medicine. 1983; 208:525-533. 5. Mana J, Salazar A, Manresa F: Clinical Factors Predicting Persistence of Activity in Sarcoidosis: A Multivariate Analysis of 193 Cases. Respiration 1994;61:219-225. 6. Sharma, OP: Pulmonary Sarcoidosis and Corticosteroids. Am Rev Respir Dis 1993;147:1598-1600. 7. Poe RH, Levy PC: Diagnosis and treatment of sarcoidosis. Comprehensive Therapy 1993;19(5):209-213. 8. Löfgren S, Stavenow S: Course and prognosis of sarcoidosis. Am Rev Resp Dis 1961;84/2:66-70. 9. Glennas A, et al.:Acute Sarcoid Arthritis: Occurrence, seasonal onset, clinical features and outcome. British Journal of Rheumatology 1995;34:45-50. 10. Lever WF, Schaumberg-Lever G: Histopathology of the Skin, seventh edition, pp 252-256. Philadelphia, JB Lippincott, 1990. 11. Goldberg, BA, Fanburg BL: Indications for Corticosteroid Use in Sarcoidosis. Hospital Physician 1996;32:11-21,51. 12. Fitzpatrick TB, et al. (ed) Dermatology in General Medicine, fourth edition, pp. 1334-1340. New York, McGraw-Hill, Inc., 1993. 13. Fitzpatrick TB, et al. (ed) Dermatology in General Medicine, fourth edition, pp. 2221-2228. New York, McGraw-Hill, Inc., 1993. |
© 1997 Dermatology Online Journal for use in electronic format, otherwise copyright is retained by the author(s) |