Foreign-body reaction with superinfection
Published Web Location
https://doi.org/10.5070/D39p470722Main Content
Foreign-body reaction with Mycobacterium abseccus superinfection
Brian R Toy MD
Dermatology Online Journal 9(4): 29
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
Mycobacterium abscessus is a rare cause of skin and soft tissue infections that often results from inoculation with contaminated foreign material. A 41-year-old woman is described regarding an outbreak of M. abscessus following soft tissue augmentation. Clinical features and treatment options are reviewed.
Clinical summary
History.—A 41-year-old Mexican woman had a 1-month history of facial lesions. She presented to the Bellevue Hospital Medical Center in June 2002 with multiple nodules on the face. The patient had soft tissue augmentation of these areas approximately 3 months prior in the home of a Venezuelan woman who identified herself as a physician. The patient believes collagen was used for the procedure, although no prior allergy testing was performed. Postoperatively there were no immediate complications. After 2 months the injected areas became painful and swollen. She went to a local emergency room. One lesion was incised and drained, and she was placed on oral antibiotics. After referral to dermatology, a biopsy was performed, and the patient was placed on oral prednisone.
On June 30, 2002, the New York City Department of Health issued an alert regarding a cluster of Mycobacterium abscessus infections after injections for cosmetic purposes [1]. All cases involved Hispanic women who received cosmetic injections in nonmedical settings between January and May 2002. Patients presented with soft tissue infections to three different hospitals in Manhattan and Queens [1]. Mycobacterium abscessus was identified in each of these patients. Since June, an additional five cases have been reported [2]. All isolates in this outbreak were susceptible to clarithromycin.
On the basis of this report, clarithromycin (500 mg twice daily) was started. After 1 month of therapy with clarithromycin, she continued to complain of painful nodules on the face. A foreign-body reaction remained a concern, as the substance used for soft-tissue augmentation was still unknown. After discussion with the infectious disease service, the patient was placed on a 1-month oral prednisone taper while continuing her antimicrobial therapy. She continues to improve and is now completing a 6-month course of clarithromycin.
On July 17, 2002, New York City police arrested the Venezuelan woman identified in this case and her husband. They were charged with assault, scheming to defraud, and practicing medicine without a license. A substance called Hyacell, a hyaluronic acid derivative used for soft-tissue augmentation, was confiscated from the accused and may have been smuggled illegally from Venezuela [2]. Investigators from the Centers for Disease Control and Prevention believe that this substance was involved in the outbreak [2].
Physical examination.—Multiple, erythematous nodules were present around the cheeks and jaw. Some were firm and painful; others were fluctuant with purulent discharge.

|
|
| Figure 1 | Figure 2 |
|---|
Laboratory data.—A skin-biopsy specimen was performed for culture of atypical mycobacteria but failed to yield any growth. Gram stain and bacterial and fungal cultures of this specimen were negative.
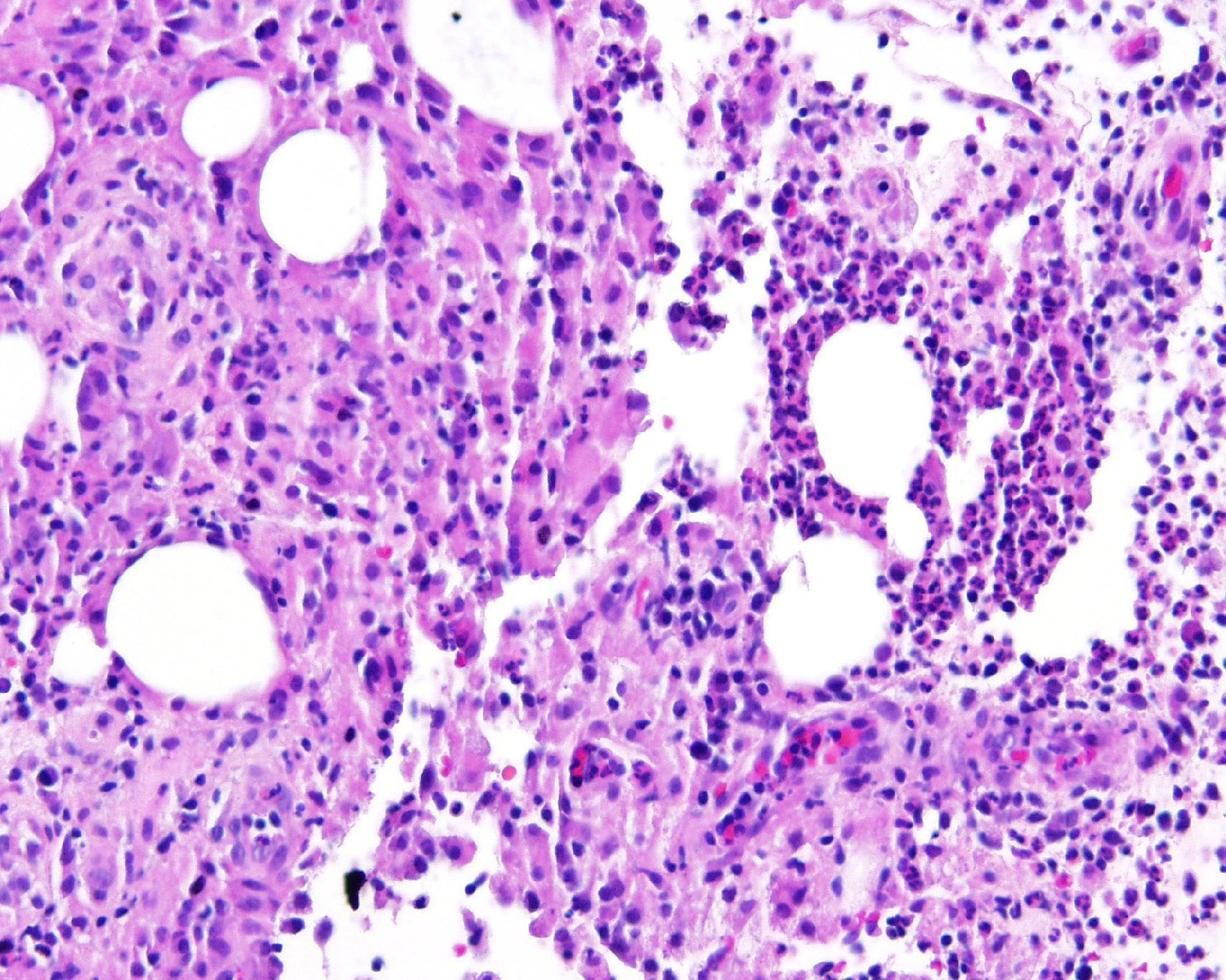
Histopathology.—There is a diffuse infiltrate composed of ill-defined granulomas and collections of neutrophilic microabscesses that involve the dermis and subcutaneous tissue. An acid-fast stain shows rare, positive-staining organisms.
Diagnosis.—Foreign-body reaction with Mycobacterium abscessus superinfection.
Comment
Mycobacterium abscessus (formerly M. chelonae subspecies abscessus) is an acid-fast, rapidly growing, nontuberculous mycobacterium. The organism is ubiquitous and is found in dust, soil, and municipal water supplies. Although it rarely causes disease in humans, M. abscessus has been associated with skin and soft-tissue infections after inoculation or puncture wounds [3]. It has also been associated with infection involving foreign material, such as prosthetic valves or joints, dialysis catheters, tympanoplasty tubes, and breast implants [4]. Disseminated infection, although rare, can cause death, particularly in immunocompromised hosts.
Treatment of M. abscessus infection involves removal of infected material and antimicrobial therapy. Most isolates of M. abscessus are susceptible to amikacin, cefoxitin, imipenem, and clarithromycin. In localized infection, clarithromycin is the drug of choice, with a 4-6 month duration of therapy [4]. However, in disseminated disease, combination therapy is recommended to prevent resistance.
References
1. Munsiff S, Adams L. 2002 Alert #14: Cluster of Mycobacterium abscessus infections following injections for cosmetic purposes. The City of New York Department of Health, June 30, 2002.2. Fries J. More illegal botox-like injections suspected. New York Times 2002 July 20;Sect. B:1,3.
3. Villanueva A, et al. Report of an outbreak of postinjection abscesses due to Mycobacterium abscessus. Clin Infect Dis 1997;24:1147.
4. Mandell G, et al. Principles and practice of infectious disease. 5th ed. New York: Churchill Livingstone; 2000, 2633.
© 2003 Dermatology Online Journal