Multiple human papillomavirus-16 associated digital squamous-cell carcinomas in an immunocompetent woman with prior human papillomavirus-related genital carcinoma
Published Web Location
https://doi.org/10.5070/D32f14k5wsMain Content
Multiple human papillomavirus-16 associated digital squamous-cell carcinomas in an immunocompetent woman with prior human
papillomavirus-related genital carcinoma
Raegan Hunt MD PhD, Charlotte Hwa BA, Julia Tzu MD, Rishi Patel MD, Peter Rady MD PhD, Stephen K Tyring MD PhD, Jennifer Stein
MD PhD
Dermatology Online Journal 17 (10): 20
Department of Dermatology, New York University, New York, New York Abstract
High-risk subtype human papillomavirus (HPV) infection, which is known to contribute to the oncogenesis of anogenital squamous-cell carcinoma (SCC), is detected in the majority of digital SCCs. Evidence suggests a genital-digital route of transmission of high-risk HPV, and most HPV-related digital SCCs occur near the nail unit in immunocompetent adults. As early HPV-related SCC commonly appears as a verrucous periungual papule, a biopsy should be considered if such a lesion persists or occurs in an individual who is likely to inoculate their digits with high-risk HPV from digital-genital contact with themselves or sexual partners. We present a 60-year-old woman, who has a personal history of vulvar and cervical SCC and an appreciable disease burden from SCCs that involved five digits of her hands.
History
A 60-year-old woman presented to the Charles C. Harris Skin and Cancer Unit for evaluation of gradually expanding verrucous plaques on five digits of the hands. The affected digits were painful and intermittently bled, and were without loss of sensation or paresthesia. She denied a history of trauma to her fingers as well as any occupational or environmental exposure to carcinogens. She reported minimal exposure to well water in Puerto Rico and no known arsenic ingestion. Past medical history included genital warts, vulvar squamous-cell carcinoma, and invasive cervical cancer, which required wide local vulvar excision, skin grafting, and hysterectomy. She reported that the growths on her fingers developed approximately ten years after the genital warts appeared. They had been treated with cryotherapy without resolution. There was no history of susceptibility to infectious organisms. She reports one lifetime male sexual partner, who also was infected with genital warts. No family members have a similar skin condition. Review of symptoms was negative.
Physical examination
 |
| Figure 1 |
|---|
Verrucous, pink-tan plaques extended from the distal phalanx to past the distal interphalangeal joint in a partially-circumferential manner on the first and second digits of the right hand and the second through fourth digits of the left hand. A 1 mm to 2 mm band of brown hyperpigmentation accentuated the proximal edges of several plaques. On three of the five affected digits, the nailplate was lost or dystrophic. The toes were normal. No verrucous, flat papules or erythematous macules were found elsewhere on the body.
Laboratory data
Radiographs of the affected fingers were unremarkable with no bony invasion. A complete blood count was normal. An ELISA test was negative for antibodies to the human immunodeficiency virus-1. Human papillomavirus (HPV) testing of the digital lesions demonstrated infection with HPV-16 [1].
Histopathology
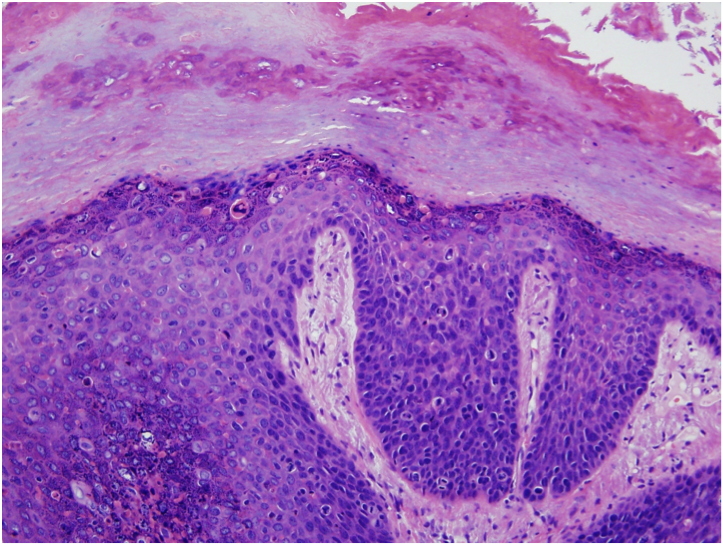 |
| Figure 2 |
|---|
There is a papillated, acanthotic epidermis with orthokeratosis and parakeratosis, full-thickness keratinocytic atypia, suprabasal mitoses, and dyskeratosis.
Discussion
Although the exact incidence is unknown, digital squamous-cell carcinoma (SCC) represents a small subset of SCC. Digital SCC can present a diagnostic challenge by mimicking benign conditions, such as verruca vulgaris and chronic paronychia. Risk factors for the development of SCC include exposure of the hands to ionizing radiation or carcinogenic chemicals, arsenic ingestion, trauma, burns, genetic predisposition from specific genodermatoses, immunosuppression, and infection with human papillomavirus (HPV) [2-7].
High-risk HPV strains (most frequently HPV-16, -18, -31, and -35) are known to contribute to oncogenesis in anogenital and cervical SCC [8]. Apart from genital SCCs, HPV-associated cutaneous SCC in the immunocompetent host has been limited to the fingers with a predilection for the periungual and subungual areas [9, 10]. Over a 15-year period, one group found that 90 percent of all digital SCCs encountered were HPV-associated. However, they noted that HPV positive and negative digital SCCs affected the same demographic population and were clinically indistinguishable [10]. The most frequent clinical presentation of HPV-related digital SCC is a persistent, periungual, verrucous papule or plaque, but also it may manifest as a subungual tumor, onycholysis, or melanonychia [11].
The most commonly associated HPV type in digital SCC is HPV-16, which accounts for 74 percent of examined cases although HPV-2, -11, -18, -26, -31, -34, -35, -56, -58, and -73 also have been detected [12]. HPV-11, which is the only associated low-risk HPV type reported, always co-existed with a high-risk HPV subtype. In some patients, the same HPV type has been identified in both digital SCCs and samples from genital dysplasia, which suggests a genital-digital transmission route [10]. A literature review of 120 HPV-associated digital SCCs found that approximately one-third of the patients had a history of HPV-related genital disease in themselves or a sexual partner, and only 6.8 percent of patients were immunocompromised. In this series, multiple HPV-related digital SCCs occurred in only thirteen patients (12.6%), among whom one patient was female [11].
HPV-related and HPV-negative digital SCCs share the same 2 percent to 3 percent risk of metastasis; however, HPV-related digital SCCs are more likely to be locally aggressive and to recur after excision [13]. In comparison to HPV-negative digital SCCs, HPV-related digital SCCs exhibit higher levels of p16INK4a and Ki67 expression, which suggests that an increased cellular proliferation rate may contribute to the biologic behavior of these tumors [9]. The majority of digital SCCs are surgically excised using the Mohs micrographic technique. HPV-related digital SCC recurrence after Mohs micrographic surgery is reported to be as high as 20 percent in contrast with an average recurrence rate of 3 percent for all cutaneous SCC after Mohs micrographic surgery [11, 14]. Residual oncogenic HPV harbored in cells beyond the tumor margin, which was observed in two cases at the periphery of the specimen, may in part account for this high recurrence risk [10]. Radiation therapy has been described as an alternative treatment modality for those unable or unwilling to undergo surgical excision [11].
References
1. Fussel Haws AL, et al. Nested PCR with the PGMY09/11 and GP5(+)/6(+) primer sets improves detection of HPV DNA in cervical samples. J Virol Methods 2004; 122: 87 [PubMed]2. Albom AJ. Squamous-cell carcinoma of the finger and nail bed: a review of the literature and treatment by the Mohs' surgical technique. J Derm Surg 1975; 1: 43 [PubMed]
3. Kopelson PL, et al. Verruca vulgaris and radiation exposure are associated with squamous cell carcinoma of the finger. J Derm Surg Oncol 1994; 20: 38 [PubMed]
4. Moy RL, et al. Human papillomavirus type 16 DNA in periungual squamous cell carcinomas. JAMA 1989; 261: 2669 [PubMed]
5. Porembski MA, Rayan GM. Subungual carcinomas in multiple digits. J Hand Surg Eur Vol 2007; 32: 547 [PubMed]
6. Chalmers RL, et al. Multiple digital squamous cell carcinoma due to 'soluble-oil'. J Plast Reconstr Aesthet Surg 2008; 61: 1147 [PubMed]
7. Drolet BA, et al. Role of human papillomavirus in cutaneous oncogenesis. Ann Plast Surg 1994; 33: 339 [PubMed]
8. Eliezri YD, et al. Occurrence of human papillomavirus type 16 DNA in cutaneous squamous and basal cell neoplasms. J Am Acad Dermatol 1990; 23: 836 [PubMed]
9. Kreuter A, et al. Diversity of human papillomavirus types in periungual squamous cell carcinoma. Br J Dermatol 2009; 161: 1262 [PubMed]
10. Alam M, et al. Human papillomavirus-associated digital squamous cell carcinoma: literature review and report of 21 new cases. J Am Acad Dermatol 2003; 48: 385 [PubMed]
11. Riddel C, et al. Ungual and periungual human papillomavirus-associated squamous cell carcinoma: a review. J Am Acad Dermatol 2011; [PubMed]
12. Forslund O, et al. A broad range of human papillomavirus types detected with a general PCR method suitable for analysis of cutaneous tumours and normal skin. J Gen Virol 1999; 80: 2437 [PubMed]
13. Brantsch KD, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol 2008; 9: 713 [PubMed]
14. Zabawski EJ, Jr., et al. Squamous cell carcinoma of the nail bed: is finger predominance another clue to etiology? A report of 5 cases. Cutis 2001; 67: 59 [PubMed]
© 2011 Dermatology Online Journal