Acute lipodermatosclerosis: an open clinical trial of stanozolol in patients unable to sustain compression therapy
Published Web Location
https://doi.org/10.5070/D36fd137ctMain Content
Acute lipodermatosclerosis: an open clinical trial of stanozolol in patients unable to sustain compression therapy
Z Đaković1, S Vesić1, J Vuković1, LJ Medenica1, MD Pavlović2
Dermatology Online Journal 14 (2): 1
1. Institute of Dermatovenereology, Clinical Center of Serbia, Belgrade, Serbia2. Department of Dermatology and Venereology, University Medical Center, Ljubljana Slovenia. mdpavlovic2004@yahoo.com
Abstract
Acute lipodermatosclerosis (ALDS) is a painful counterpart of chronic lipodermatosclerosis (LDS) resulting from venous insufficiency. Severe pain is the leading symptom and many patients with ALDS are unable to tolerate compression therapy. We evaluated clinical efficacy of stanozolol (2 mg bid for 8 weeks) for the reduction of pain and dermal-thickness in 17 patients with ALDS. All patients had superficial venous insufficiency documented by duplex scans, and in all of them incompetent perforators were found under the area of ALDS. Mean pain scores prior to institution of stanozolol (7±2; range 4-10) lowered significantly at the end of the 8-week treatment (3±2; range 0-5, p<0.001). Dermal thickness was also significantly reduced (p<0.01) over the treatment period. Side effects were not noted. Stanozolol, given over 8 weeks, effectively and safely alleviates pain and reduces dermal thickness in patients with ALDS.
Acute lipodermatosclerosis (ALDS) is a form of lobular panniculitis presenting as extremely painful and inflamed, red or purple, poorly demarcated plaques, often with indurated and edematous skin of the medial calf [1, 2]. Often it is misdiagnosed as cellulitis, morphea, or phlebitis. Acute lipodermatosclerosis is attributed to venous insufficiency or, less commonly, to chronic lymphedema [1, 3]. Clinical and experimental observations suggest that lipodermatosclerosis is causally related to the microangiopathy and perfusion disturbance in chronic venous insufficiency [2, 5]. Excruciating pain is a major symptom in these patients who often cannot withstand compression bandages or stockings [2]. Stanozolol, a synthetic derivative of testosterone, is a potent fibrinolytic agent that has been used successfully in the treatment of lipodermatosclerosis and venous insufficiency [1, 6, 8].
In this study we looked at the effect of stanozolol on subjective and objective signs in patients with ALDS who refused to wear either compression bandages or stockings because of the extreme pain they induced.
Methods
Upon approval of the Institutional Review Board, seventeen patients were enrolled (9 females and 8 males, aged 39-62 years, mean age 52 years) presenting with an acute-onset (within a few days prior to referral) severe pain localized to the lower third of a leg and accompanied by redness, burning sensation and tenderness. Clinical diagnosis of ALDS was made according to the diagnostic criteria proposed by Greenberg et al. [2] as follows: (a) persistent pain, tenderness and redness of the medial aspect of the leg; (b) no local or systemic evidence of cellulitis; (c) no evidence of phlebitis; and (d) clinical findings inconsistent with other types of panniculitis or with morphea. All patients had similar cutaneous lesions consisting of tender erythematous plaques and indurated skin at the lower third of a leg, mostly confined to the medial calf area. They were afebrile, and physical examination did not disclose findings suggestive of other skin or systemic disorders. Laboratory evaluaton (ESR, C-reactive protein, CBC count, blood glucose, serum lipids, liver and kidney function tests, anti-streptolysin titer, and antinuclear antibodies) was within normal limits. All patients refused to be biopsied and the diagnosis of ALDS was made on clinical and (unrevealing) laboratory findings. According to the CEAP (Clinical, Etiologic, Anatomic, Pathophysiologic) classification, 15 patients belonged to the C3 and 2 patients to the C4 group (the two patients already treated for venous varicosities with graduated compression and, by history, had some degree of hyperpigmentation and slight cutaneous sclerosis—concealed by the acute cutaneous changes. Although most patients were overweight, only 3 of them had BMIs higher than 30 (obese). Upon obtaining an informed consent, whole leg duplex mapping was performed by a single radiologist evaluating deep and superficial venous system for patency, patterns of reflux, and anatomic layout using a linear 7.5 MHz transducer (Toshiba Powervision 6000, Otawara, Japan). Patients were examined sitting and standing with the leg not weight bearing, and reflux was assessed segment by segment using distal compression release.
All patients refused to apply either compression bandages or stockings or cold wet compresses because of severe pain induced even by a gentle touch of the affected skin. They were immediately given stanozolol, 2 mg BID, and instructed to bed rest and leg elevation as much as possible for 8 weeks. Analgetic drugs were not allowed. Blood pressure was monitored daily, and liver and kidney function tests every 4 weeks. Pain intensity was measured by a visual numeric scale (VNS), an 11-point numeric rating scale for pain (NRS-11); patients were asked to choose a number on a scale from 0 (no pain) to 10 (worst pain you can imagine), prior to and after 2 months of therapy with stanozolol [9]. Erythema was scored semiquantitatively (0, no erythema; 1, mild erythema; 2, moderate erythema; 3, severe erythema). Dermal thickness was measured by a high-resolution ultrasound device (20 MHz, DermaScan C, Cortex Technology, Hadsund, Denmark) prior to and after stanozolol treatment on the affected (3 cm above the center of the medial malleolus) and clinically healthy skin of the lower leg. Maximum depth of the ultrasound signal was 10 mm and the width of the measured area was 12 mm. Thickness of the skin was calculated in B-mode outlining the image of a whole skin block with a cursor by hand on the screen, excluding the hyperechogenic entrance echo and the hypoechogenic subcutis. A pronounced dermal edema in ALDS gave a subepidermal low echogenic band interposed between the entrance echo and the residual dermal echo signal.
The software SPSS 9.0 (StatSoft Inc., USA) was used for all calculations and analyses. Erythema scores and NRS-11 were compared at the start and at the end of the treatment using Wilcoxon Z-test for dependent samples, whereas dermal thickness values were compared with Student's t-test for two dependent samples. The level of significance was set at p less than 0.01. Linear regression was used to assess the relationship between dermal thickness prior to and after the treatment.
Results
In all patients, duplex ultrasonography confirmed the presence of superficial venous insufficiency—segmental or truncal greater saphenous vein reflux in 7 legs, small saphenous vein reflux in 6 legs, and incompetent medial leg perforating veins were found under the area of ALDS in all 17 legs. Deep veins were patent and functional in all patients.
 |
| Figure 1 |
|---|
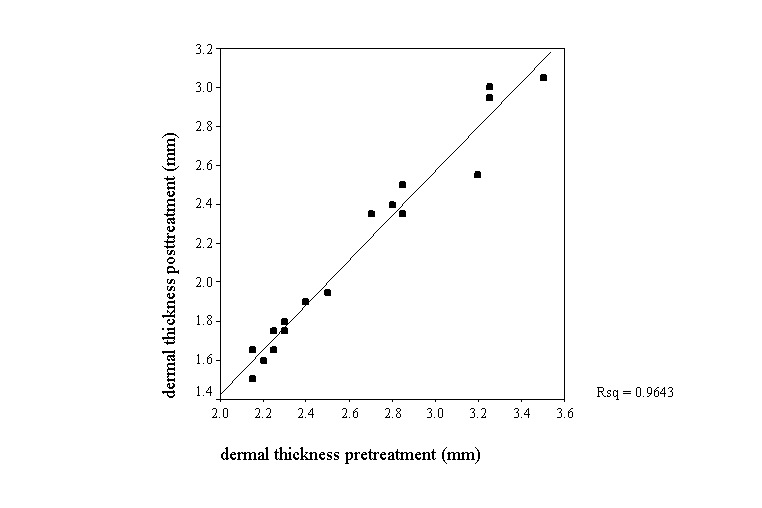
| Figure 1. Linear correlation of dermal thickness (mm) before and after stanozolol treatment |
Mean pain and erythema scores in patients with ALDS decreased significantly over the 8-week treatment with stanozolol (Table 1, p<0.001). The pain alleviation was significant already after 4 weeks of the therapy. The subjective improvement was also reflected in a significant reduction of dermal thickness of the affected lower leg, from a mean 2.64 mm to 2.15 mm (Table 1; P<0.01). Linear regression analysis showed that there is a linear correlation of dermal thickness values before and after stanozolol treatment with a coefficient of determination (R2) 96.4 percent (Fig. 1). At the end of the treatment, all patients were able to tolerate compression bandages. During the study, we did not encounter a single side effect of stanozolol treatment. Blood pressure, liver function tests and serum lipid levels did not change significantly.
Discussion
Acute lipodermatosclerosis is a sign of chronic venous insufficency and some authors consider it a part of the post-phlebitic syndrome [1, 2, 10]. Histologically, it is mostly lobular panniculitis with increased sclerosis in fat and areas of membranous fat necrosis and fat microcysts [11]. The lesions usually last for several months but may persist for more than a year and develop into more common, chronic LDS. Available evidence suggests that prolonged venous hypertension induces damage to dermal capillaries allowing large molecules such as fibrinogen to leak into the dermis. Moreover, patients with LDS may produce lower levels of plasminogen activator coupled with a simultaneous presence of elevated levels of its inhibitors in blood and tissues [12].
The main complaint of patients with ALDS is severe unremitting pain accompanied by extreme skin sensitivity. The pain sensation may prevent application of compression, the first-line treatment option for this condition and venous insufficiency in general. Topical capsaicin has been shown very effective in the treatment of ALDS in 3 patients [13]. Stanozolol, an anabolic steroid, exerts a potent fibrinolytic action [7]. Increased fibrinolysis in skin lesions and reduction in pain has been shown in a 6-month double-blind trial using stanozolol in patients with venous insufficiency and the chronic form of LDS [8]. In their review, Helfman and Falanga [7] described the efficacy of stanozolol also in patients with ALDS stating that within weeks pain is remarkably reduced, and by 2-3 months the skin becomes less indurated. Yet, except for single case reports [14], there are no published clinical trials on the efficacy of stanozolol in ALDS. Our results confirm that stanozolol is an efficacious agent in relieving pain, and reducing erythema and dermal thickness in patients with ALDS (Table 1, Fig. 1). The relatively short-term administration of stanozolol reduces the chance of development its side effects, primarily liver toxicity. In addition, duplex investigation in our patients confirms that ALDS almost always develops in the setting of venous insufficiency.
This small open trial might be criticized for two major drawbacks. First, there was no histologic confirmation of ALDS, and, secondly, the lack of a control group of ALDS patients who would not receive any specific treatment, except for bed rest and leg elevation. The patients declined the biopsy because of great skin tenderness. A combination of clinical and laboratory data (see the Methods section) was used to exclude other possible conditions, such as cellulitis, phlebitis, and morphea. Because patients were not allowed to take analgesic medications and could not wear compression bandages, it was deemed unethical leaving a group of them without any specific treatment, especially in light of positive results obtained with stanozolol in subjects with chronic lipodermatosclerosis [6]. Because ALDS forces its sufferers to abstain from walking or bearing weight on the affected leg, even prior to their presentation they will frequently find ways of staying off their feet. In two placebo-controlled trials of stanozolol in chronic LDS all the patients wore compression stockings [6, 8]. In a recent case series it was stated that 32 percent of patients with chronic lipodermatosclerosis do not have a venous abnormality, but are either overweight or obese [15]. This is in contrast with findings of Greenberg et al. [2] who confirmed the presence venous insufficiency in all of their patients with ALDS. It seems that a subset of patients have no apparent venous abnormalities, suggesting pathophysiological mechanisms not simply related to stasis. These patients are often overweight or obese. Bruce et al [15] proposed that venous hypertension might be the linking pathogenic key factor for both groups of patients.
Though the open clinical trial has obvious limitations, the results support the use of stanozolol in patients with ALDS, especially when they cannot tolerate compression therapy. After several weeks of treatment, most patients experience significant pain moderation and are able to wear compression bandages or stockings.
References
1. Kirsner RS, Pardes JB, Eaglstein WH, Falanga V. The clinical spectrum of lipodermatosclerosis. J Am Acad Dermatol. 1993 Apr;28(4):623-7. PubMed2. Greenberg AS, Hasan A, Montalvo BM, Falabella A, Falanga V. Acute lipodermatosclerosis is associated with venous insufficiency. J Am Acad Dermatol. 1996 Oct;35(4):566-8. PubMed
3. Gniadecka M. Localization of dermal edema in lipodermatosclerosis, lymphedema, and cardiac insufficiency. High-frequency ultrasound examination of intradermal echogenicity. J Am Acad Dermatol. 1996 Jul;35(1):37-41. PubMed
4. Bull RH, Mortimer PS. Acute lipodermatosclerosis in a pendulous abdomen. Clin Exp Dermatol. 1993 Mar;18(2):164-6. PubMed
5. Howlader MH, Smith PD. Microangiopathy in chronic venous insufficiency: quantitative assessment by capillary microscopy. Eur J Vasc Endovasc Surg. 2003 Sep;26(3):325-31. PubMed
6. Burnard K, Clemenson G, Morland M, Jarrett PEM, Browse NL. Venous lipodermatosclerosis, treatment by fibrinolytic enhancement and elastic compression. Br Med J. 1980 Jan 5;280(6206):7-11. PubMed
7. Helfman T, FalangaV. Stanozolol as a novel therapeutic agent in dermatology. J Am Acad Dermatol. 1995 Aug;33(2 Pt 1):254-8. PubMed
8. McMullin GM, Watkin GT, Coleridge Smith PD, Scurr JH. Efficacy of fibrinolytic enhancement with stanozolol in treatment of venous insufficiency. Aust N Z J Surg. 1991 Apr;61(4):306-9. PubMed
9. Kendrick DB, Strout TD. The minimum clinically significant difference in patient-assigned numeric scores for pain. Am J Emerg Med. 2005 Nov;23(7):828-32. PubMed
10. Ryan TJ, Burnard KG. Diseases of the veins and arteries: leg ulcers. In: Rook et al. Textbook of Dermatology, 6th ed, eds: Champion RH et al, Blackwell, Oxford, 1998: 2228-76.
11. Requena L, Yus ES. Panniculitis. Part II Mostly lobular panniculitis. J Am Acad Dermatol. 2001 Sep;45(3):325-61. PubMed
12. Peschen M, Rogers MM, Chen WY, et al. Modulation of urokinase type and tissue type plasminogen activator occurs at an early stage of progressing stages of chronic venous insufficiency. Acta Derm Venereol. 2000 May;80(3):162-6. PubMed
13. Yosipovitch G, Mengesha Y, Facliaru D. Topical capsaicin for the treatment of acute lipodermatosclerosis and lobular panniculitis. J Dermatolog Treat. 2005 Aug;16(3):178-80. PubMed
14. Hafner C, Wimmershoff M, Landthaler M, Vogt T. Lipodermatosclerosis: successful treatment with danazol. Acta Derm Venereol. 2005;85(4):365-6. PubMed
15. Bruce AJ, Bennett DD, Lohse CM, Rooke TW, Davis MDP. Lipodermatosclerosis: review of cases evaluated at Mayo Clinic. J Am Acad Dermatol. 2002 Feb;46(2):187-92. PubMed
© 2008 Dermatology Online Journal