Scaly scalp associated with crusted scabies: Case series
Published Web Location
https://doi.org/10.5070/D37s8396g0Main Content
Scaly scalp associated with crusted scabies: Case series
TS Anbar MD, MB El-Domyati MD, HA Mansour MD, HM Ahmad MD
Dermatology Online Journal 13 (3): 18
Department of Dermatology, Faculty of Medicine, Al-Minya University, Al-Minya, Egypt. taganbar@yahoo.comAbstract
The diagnosis of crusted scabies is becoming more relevant due to the increase in number of immunocompromised patients. To date, more than 200 cases have been reported in the literature. However, crusted scabies seems to be under-diagnosed because of its unusual presentations. In this case series we present history, clinical manifestations, KOH smear, and histopathological findings of a series of four patients with crusted scabies. Scaly scalp was a prominent feature of the disease in all cases. Examination of and treatment of the scalp of patients with suspected crusted scabies should not be neglected. A KOH smear from the scalp offers a simple and reliable technique for diagnosis.
Crusted scabies, a rare variant of scabies, is a highly contagious condition in which the skin is heavily infested with mites, Sarcoptes scabiei var hominis [1]. This condition has been reported in patients with leprosy [2], autoimmune diseases, malnutrition, mental disability, Down syndrome [3], and immune compromise [1]. Additional cases have occurred after inappropriate use of potent fluorinated corticosteroids [4]. However, in some patients, no identifiable risk factor can be detected [2].
To date, more than 200 cases of crusted scabies have been reported in the literature [1]. Many times, the diagnosis is delayed or missed because of the atypical features; it is likely much more common than reported [5].
Crusted scabies rarely presents with scalp involvement [5, 6, 7, 8]. We present a series of four patients with crusted scabies in whom scaly scalp was an evident component of the disease.
Case series
Case 1
An 8-year-old boy with a moderate degree of mental retardation presented with large, warty, crusted plaques of 1-year duration (Fig. 1). The lesions were seen on the scalp, breasts, axillae, buttocks, penis, palms, and soles. Masses of horny debris accumulated beneath the thickened nails (subungual hyperkeratosis).
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Case no. 1: Large warty crusted lesions over breasts and axillae (A) and palms (B). CLICK for full image. Figure 2. Case no. 2: Thick hyperkeratotic plaques on the anterior axillary folds and antecubital fossae and widespread papular eruption over the trunk (A). Large irregular fissured thick hyperkeratotic plaques on the face (B). | |
Case 2
A 25-year-old woman presented with a 2-month history of large, irregular, fissured, hyperkeratotic plaques on the scalp, face, neck, trunk, anterior axillary folds, anticubital fossae, palms, peri-umbilical region, and upper half of the thighs (Fig. 2).
Case 3
A 20-year-old woman with a mild degree of mental retardation presented with crusted lesions over the face, neck, trunk, buttocks, and scalp (Fig.3); she had experienced mild itching for 1 month. The patient was taking low-dose systemic corticosteroid therapy for systemic lupus erythematosus.
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Case no. 3: Crusted lesions over the face, neck and chest (A) together with scaly scalp (B) Figure 4. Case no. 4: Bilateral symmetrical psoriasiform crusted hyperkeratotic plaques on the neck, breasts, axillary folds and antecubital fossae together with multiple vitiliginous lesions (A). Dorsa of hands were irregularly thickened and fissured (B). | |
Case 4
An 18-year-old woman presented with bilateral, symmetrical, psoriasiform, hyperkeratotic plaques of 20-days duration (Fig. 4). The plaques were seen on the scalp, neck, breasts, axillary folds, wrists, and elbows. The dorsa of hands were irregularly thickened and fissured. Subungual hyperkeratosis was also evident. Multiple vitiliginous macules were noted over different parts of the body. The patient was receiving systemic corticosteroid therapy as a treatment for vitiligo.
 |  |
| Figure 5 | Figure 6 |
|---|---|
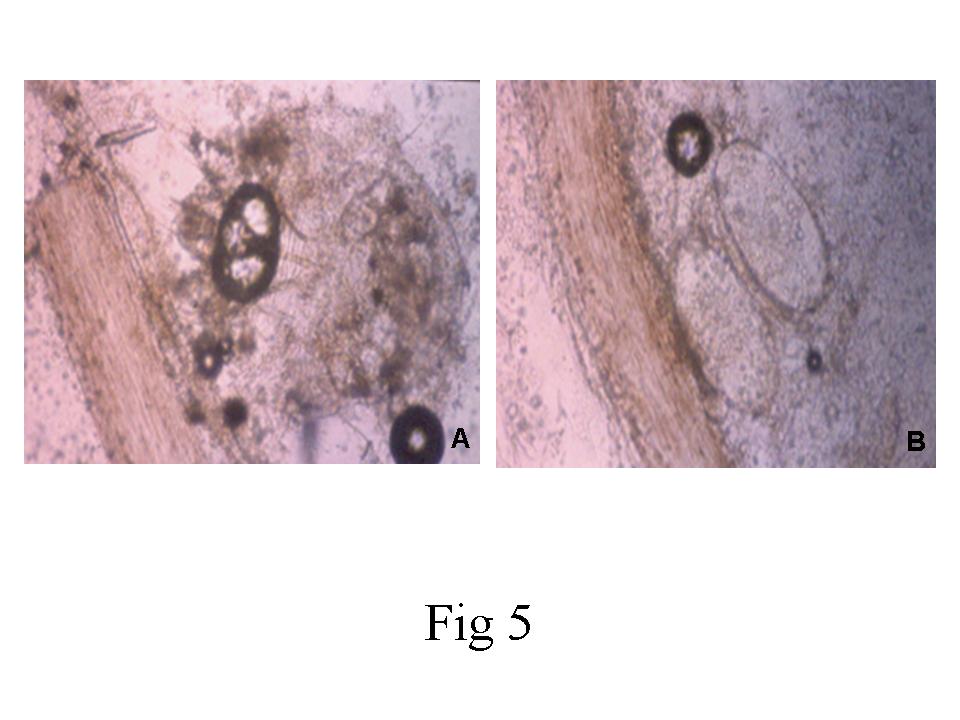
| Figure 5. KOH smear from scalp showing adult mites (A) & eggs (B) of Sarcoptes Scabiei closely attached to the hair shaft
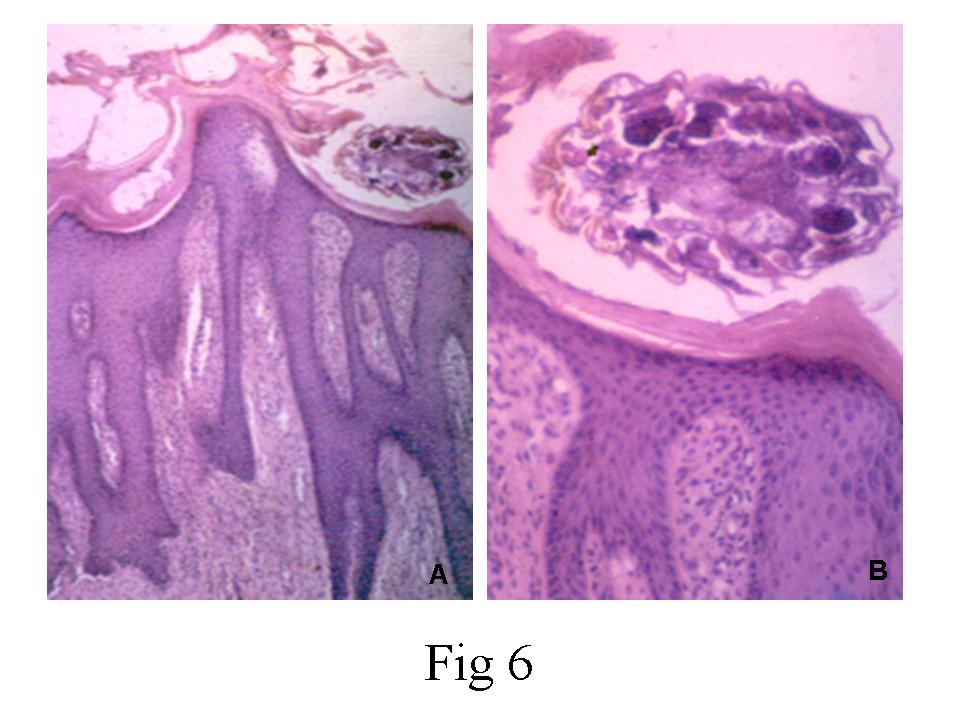
(Oil immersion; original magnification X100) Figure 6. A mite of Sarcoptes Scabiei is seen in the scale crust. A dense mixed inflammatory cell infiltrate is noted beneath the hyperplastic epidermis. (H & E; original magnification X20 (A) and X40 (B). | |
It is worthy to note that HIV screening with ELISA test was negative in all patients. Skin scrapings and KOH smear from skin lesions as well as from scalp showed adult mites and eggs of Sarcoptes scabiei in all cases (Fig. 5). In addition, skin biopsies from the lesions showed numerous mites throughout the scale crust in all cases (Fig. 6). A dense, mixed-inflammatory-cell infiltrate was noted beneath the hyperplastic epidermis.
Discussion
Scabies is a common, very contagious, highly pruritic infestation of the skin associated with Sarcoptes scabiei var hominis. An infested patient my exhibit specific lesions, such as burrows, and non-specific lesions, such as papules, vesicles, and excoriations. Typically affected areas are the finger webs, wrists, axillary folds, abdomen, buttocks, infra-mammary folds and male genitalia [9,10].
Crusted scabies is a generalized severe form of the infestation usually presenting with a cutaneous eruption of hyperkeratotic and crusted papules and plaques [11]. Burrows, commonly found on the hands, wrists, ankles, and interdigital areas, are less apparent. Moreover, lesions may be generalized with subungual debris and gross nail thickening attributed to an extraordinary mite load [12].
The definitive diagnosis of scabies is made when the scabies mites or their eggs or fecal pellets are identified by light microscopy [9]. In all of the present cases, KOH smears were positive in scrapings obtained from skin as well as scalp. This suggests that KOH smear, being a simple bedside test, can provide a quick and reliable diagnosis in suspected cases of crusted scabies.
Because cutaneous features in the scalp area among adult patients are rarely considered as a manifestation of scabies [5], the scalp area is often overlooked during routine clinical examination. In addition, because of the common belief that scabies does not infest the scalp, this area may be neglected during treatment, leading to treatment failures.
In conclusion, scaly scalp is an important feature in the diagnosis of crusted scabies. A KOH smear from the affected scalp is a quick, simple, and reliable diagnostic tool to identify the adult mites and/or their ova. Whenever there is a possibility of scalp involvement, this area must also receive adequate treatment.
References
1. Guldbakke KK, Khachemoune A. Crusted scabies: a clinical review. J Drugs Dermatol. 2006 Mar; 5(3): 221- 7.2. Roberts LJ, Huffam SE, Walton SF, Currie BJ. Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature. J Infect. 2005 Jun; 50(5): 375- 81.
3. Ndiaye B, Develoux M, Dieng MT. Crusted (Norwegian) scabies in Dakar (Senegal). Sante. 1999 Jul-Aug; 9(4): 243- 8.
4. Marliere V, Roul S, Labreze C, Taieb A. Crusted (Norwegian) scabies induced by use of topical corticosteroids and treated successfully with ivermectin. J Pediatr. 1999 Jul; 135(1): 122- 4.
5. Grabowski G, Kanhai A, Grabowski R, Holewinski J, Williams ML. Norwegian scabies in the immunocompromised patient. J Am Podiatr Med Assoc. 2004 Nov-Dec; 94(6): 583- 6.
6. Dourmishev AL, Serafimova DK, Dourmishev LA, Mualla MA, Papaharalambous V, Malchevsky T. Crusted scabies of the scalp in dermatomyositis patients: three cases treated with oral ivermectin. Int J Dermatol. 1998 Mar; 37(3): 231- 4.
7. Farrell AM, Ross JS, Bunker CB, Staughton RC. Crusted scabies with scalp involvement in HIV-1 infection. Br J Dermatol. 1998 Jan; 138(1): 192- 3.
8. Lewis EJ, Connolly SB, Crutchfield CE 3rd, Rest EB. Localized crusted scabies of the scalp and feet. Cutis. 1998 Feb; 61(2): 87- 8.
9. Chouela E, Abeldano A, Pellerano G, Hernandez MI. Diagnosis and treatment of scabies: a practical guide. Am J Clin Dermatol. 2002; 3(1): 9- 18.
10. Flinders DC, De Schweinitz P. Pediculosis and scabies. Am Fam Physician. 2004 Jan 15; 69(2): 341- 8.
11. Schlesinger I, Oelrich M, Tyring SK. Crusted (Norwegian) scabies in patients with AIDS: the range of clinical presentations. South Med J. 1994;87:352-6.
12. Orkin M. Scabies in AIDS. Semin Dermatol. 1993;12:9-14.
© 2007 Dermatology Online Journal