Clinical and histopathological improvement of psoriasis with oral chondroitin sulfate: A serendipitous finding
Published Web Location
https://doi.org/10.5070/D32zh8x3vfMain Content
Clinical and histopathological improvement of psoriasis with oral chondroitin sulfate: A serendipitous finding
Josep Vergés MD PhD1, Eulàlia Montell PhD1, Marta Herrero BScPharm1, Cristian Perna MD2, Jesús Cuevas MD PhD2, Joan Dalmau MD3, Montserrat Pérez MD PhD3, and Ingrid Möller MD4
Dermatology Online Journal 11 (1): 31
1. Clinical Research Unit, Scientific Medical Department, Bioibérica, S.A., Barcelona, Spain. jverges@bioiberica.com2. Department
of Pathology, Hospital General Universitario de Guadalajara, Guadalajara, Spain 3. Service of Dermatology, Hospital de la
Santa Creu i Sant Pau, Barcelona, Spain 4. Instituto Poal de Reumatología, Barcelona, Spain
Abstract
We describe the clinical and histopathological results of plaque psoriasis in eleven adult patients with knee osteoarthritis and long-standing, moderate to severe psoriasis resistant to conventional therapy treated with chondroitin sulfate. Patients received 800 mg per day of chondroitin sulfate for 2 months. Skin biopsies were obtained before and after treatment. All patients but one presented a dramatic improvement of the condition of the skin, with a reduction of swelling, redness, flaking, and itching (clearance of psoriasis in one patient), increase in the hydration and softening of the skin, and amelioration of scaling. Histopathologically, there was a statistically significant decrease in epidermal thickness, a decrease in the thickness between the stratum basale and the stratum granulosum, a significant improvement of the degree of psoriasis activity, and a decrease in the number of keratinocytes stained with Ki-67. The confirmation of these serendipitous findings in controlled prospective studies could represent an important advance in the therapeutic armamentarium for patients with psoriasis given the excellent safety profile of chondroitin sulfate.
Introduction
Chondroitin sulfate is effective for the treatment of knee osteoarthritis [1]. The substance is a natural glycosaminoglycan that is present predominantly in the extracellular matrix surrounding cells and is most abundant in the cartilage, skin, blood vessels, ligaments, and tendons. Glycosaminoglycans of the articular cartilage constitute high-molecular-weight aggregates (proteoglycans) that contribute to the mechanical and elastic properties of this structure [2]. The therapeutic effect of chondroitin sulfate shown in patients with osteoarthritis is probably the result of its anti-inflammatory activity, stimulation of the synthesis of proteoglycans and hyaluronic acid, decrease of the catabolic activity of chondrocytes inhibiting some proteolytic enzymes and other substances that contribute to damage the cartilaginous matrix, reduction of the synthesis of nitric oxide, and apoptosis of articular chondrocytes [3, 4, 5]. Controlled clinical trials in patients with osteoarthritis show good efficacy of chondroitin sulfate, improving the symptomatology and the functional variables significantly compared to placebo [6, 7, 8]. Chondroitin sulfate promotes the modification of the clinical picture of osteoarthritis acting as a symptomatic slow-acting drug [9, 10].
In the course of the prescription of chondroitin sulfate as a symptomatic treatment for knee osteoarthritis, it was observed that patients who had a concomitant psoriasis experienced a surprisingly marked improvement of their psoriatic plaques a few days after the commencement of treatment. No information is available on the effect of this systemic medication for patients suffering from psoriasis.
Therefore, in the present study we evaluated the clinical characteristics and histopathological parameters of patients with knee osteoarthritis and psoriasis treated with oral chondroitin sulfate for the amelioration of articular symptoms.
Methods
Study design
Our study group was composed of eleven nonconsecutive adults with history of psoriasis and bilateral femorotibial osteoarthritis diagnosed according to criteria of the American College of Rheumatology [11], who were prescribed treatment with chondroitin sulfate because of persistent pain in the knee especially on motion and because of functional disability. Patients received oral chondroitin sulfate (Condro.san®, Bioiberica S.A., Barcelona, Spain), 800 mg daily (2-400 mg capsules once a day). The duration of the treatment was 2 months. Three of these patients have been previously reported in a former publication [12].
After full explanation of a possible unproved beneficial effect of the chondroprotective treatment on pre-existing psoriasis, patients volunteered to take part in the study and were referred to a dermatologist for evaluation. Patients gave written informed consent before inclusion in the study. All clinical examinations were carried out by one of the authors. Biopsy specimens were taken at baseline and after completing the course of treatment with chondroitin sulfate. All patients had a history of long-standing disabling psoriasis without clinically significant improvement with the use of phototherapy, systemic agents, or multiple topical treatments. Moderate to severe psoriasis was defined as psoriasis on more than 10 percent of the body surface, or disease that causes difficulty in at least three of the following four activities: standing, use of hands, sitting for long periods, or sleeping. None of the patients had received systemic treatment during the preceding 6 months. At the time of the study, four patients used topical treatment, including calcipotriene, betamethasone dipropionate ointment, hydration cream with 10 percent urea, and magisterial formulations. Topical treatment had to be discontinued at least 2 weeks before study enrollment.
Biopsies and staining procedures
Punch biopsy specimens of 4 mm were taken under local anesthesia with mepivacaine 1 percent before and after treatment with chondroitin sulfate from the same psoriatic plaque for each individual patient. All biopsies were examined by two independent pathologists who were unaware of the purpose of the study, origin of the biopsy specimens, and the patients' medical history. Hematoxylin and eosin staining of formalin-fixed tissue was performed using standard techniques. Biopsies were examined immunohistochemically for reactivity with Ki-67 using the alkaline phosphatase-anti-alkaline phosphatase method.
The following histologic parameters were assessed: epidermal thickness, thickness from the stratum basale to the stratum granulosum, stratum corneum thickness, keratinocyte proliferation index, presence of orthokeratotic or parakeratotic keratinization, and degree of psoriasis activity. The parameters of thickness were measured with an ocular micrometer. Proliferation index was assessed using inmunohistochemistry for the detection of Ki-67 (Zymed, San Francisco). The number of positive nuclei per field of 0.95 mm² was measured. Psoriasis activity was assessed according to the presence of diagnostic hallmarks of psoriasis, such as epidermal hyperplasia, hyperkeratosis with parakeratosis, neutrophilic exocytosis, and vascular tortuosity of superficial capillary plexus. A semi-quantitative score on a 4-point scale was used, 0 = no disease activity; 1 = mild activity, 2 = moderate activity, and 3 = pronounced activity. In two cases in which activity was difficult to asses (Cases 2 and 10), intermediate values were used.
Statistical analysis
Data analysis was done with the application SPSS for Windows (Version 9.0). The Kolmogorov-Smirnov test was used to assess normal distribution of data. Differences in the histologic parameters before and after 2-month's treatment with chondroitin sulfate were analyzed with the Student's paired t test. Results are expressed as means ± standard deviation (SD). A p value of < .05 was considered statistically significant.
Results
There were five women and six men, with a mean age of 52 ± 16 (range 39-67). Age at onset of psoriasis ranged between 16 and 38. All patients had moderate to severe plaque psoriasis and one patient (Case 1) had also an inverse psoriasis involving folds of the neck and submammary area. The disease had been present for a mean of 26 years and the maximal body surface involved during the course of the disease varied between 35 percent to 75 percent. A family association was present in three patients (27.3 %). Psoriasis triggers, including recurrent pharyngotonsillitis and emotional stress were recorded in three patients. None of the patients had psoriatic arthritis. Demographic and clinical data are summarized in Table I.
|
|
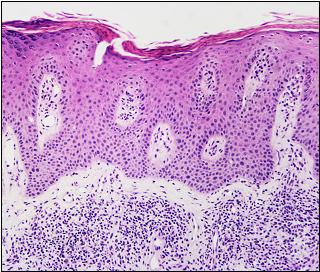
| Figure 1 | Figure 1A |
|---|---|
| Figure 1. Case 1: Epidermal thickness and inflammatory cells in a biopsy taken before treatment (hematoxylin & eosin; original magnification x30). | |
| Figure 1A. Case 1: Decrease in epidermal thickness and in the density of the inflammatory cells after treatment of chondroitin sulfate (hematoxylin & eosin; original magnification x30). | |
|
|
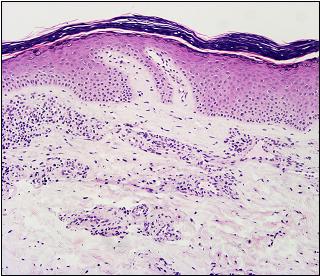
| Figure 2 | Figure 2A |
|---|---|
| Figure 2. Case 2: Vascular turtuosity in the upper superficial dermis before treatment (hematoxylin & eosin; original magnification x80). | |
| Figure 2A: Case 2: Reduction of the vascular tortuosity in the upper superficial dermis (hematoxylin & eosin; original magnification x80). | |

|
|
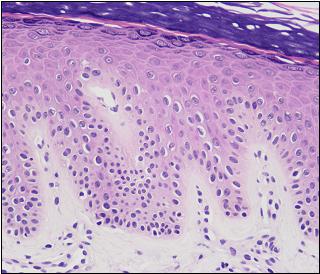
| Figure 3 | Figure 3A |
|---|---|
| Figure 3. Case 2: Stratum corneum thickness and parakeratosis before treatment with chondroitin sulfate (hematoxylin & eosin; original magnification x30). | |
| Figure 3A. Case 2: Decrease in stratum thickness and change from parakeratosis to orthokeratosis after treatment with chrondroitin sulfate (hematoxylin & eosin; original magnification x30). | |
|
|
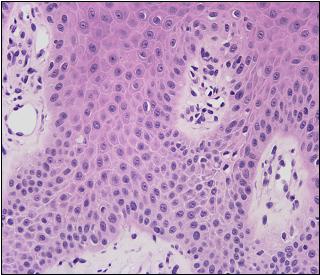
| Figure 4 | Figure 4A |
|---|---|
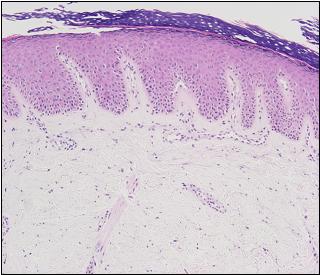
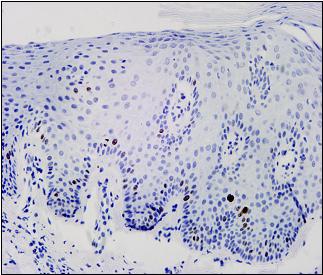
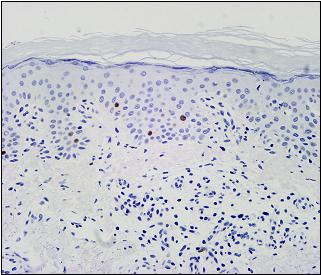
| Figure 4. Case 3: Keratinocyte proliferation index (nuclei stained with Ki-67 antibody) (original magnification x60). | |
| Figure 4A: Case 3: Decrease of the keratinocyte proliferation index (nuclei stained with Ki-67 antibody) (original magnification x60). | |
With the use of chondroitin sulfate, all patients but one (Case 7) reported a dramatic increase in the hydration of the lesions, a decrease in the flare and burning sensation as well as a marked improvement in the desquamation and the hyperkeratotic components of the lesions. In some patients, improvement was already evident after a few days of treatment. Clinical changes associated with the administration of chondroitin sulfate are described in Table I. In one patient (Case 2), hyperkeratosis almost disappeared and lesions cleared. In all patients, between 1 and 2 months after termination of treatment with chondroitin sulfate, the psoriatic lesions worsened; the patients returned to their pretreatment conditions.
Individual histopathologic data before and after treatment with chondroitin sulfate are shown in Table II.
Figures 1-3 illustrate the skin histopathological changes in three subjects who experienced a dramatic improvement. Epidermal thickness decreased from a pretreatment mean value of 396 ± 78 µm (range 300-496 µm) to 279 ± 100 µm (range 156-440 µm) after treatment (t = 3.807, p = .003), with a mean difference of 29 percent. The stratum basale to stratum granulosum thickness also decreased significantly, from 311 ± 71 µm (range 196-400 µm) to 206 ± 77 µm (range 104-344 m) after treatment (t = 3.781, p = .004), with a mean difference of 31 percent. Stratum corneum thickness tended to decrease from 99 ± 42 µm (range 32-160 µm) to 78 ± 41 µm (range 28-160 m) after treatment, but the difference was not statistically significant. Stratum corneum thickness was reduced by an average 15 percent.
On the other hand, the number of keratinocytes stained with Ki-67 decreased significantly from 33.9 ± 5.9 (range 17-45) to 25.1 ± 11.0 (range 6-40) (t = 3.170, p = .01), with a mean difference of 26 percent.
Figure 4 shows the keratinocyte proliferation reduction in case 3. The degree of psoriasis activity also improved significantly from 1.73 ± 0.68 (range 0.5-2) to 0.90 ± 0.74 (range 0-2) (t = 3.846, p = .003), with a mean difference of 49 percent.
At baseline, nine patients had extensive parakeratotic keratinization and two patients showed orthokeratotic keratinization predominantly with focal areas of parakeratosis. After completing treatment with chondroitin sulfate, all patients but three presented orthokeratotic keratinization (Table II).
Tolerability of chondroitin sulfate was excellent and none of the patients reported any adverse event.
Conclusions
In the present series of eleven patients with long-standing psoriasis in which different therapeutic modalities including systemic medications and multiple topical treatments had not been completely effective, the administration of chondroitin sulfate (800 mg daily for 2 months) was associated with a marked improvement of psoriatic plaques both clinically and histopathologically in 91 percent of cases. A single patient (Case 7) was unresponsive to chondroitin sulfate, however during chondroitin sulfate therapy, the flares, the severity of lesions at the affected sites, the psoriasis activity and proliferation of keratinocytes did not progress. The reason for the lack of response in this case is unknown. The remaining ten patients, showed a dramatic improvement of the condition of the skin with a reduction of swelling, redness, flaking, and itching. In one patient (Case 2) in whom no previous treatment produced remission of psoriasis, clearance of psoriatic plaques was observed. All patients reported an increase in the hydration and softening of the skin, amelioration of scaling, and manifested to be very satisfied with the results of treatment. More importantly, results of the histopathological study of the skin biopsies showed a statistically significant decrease in epidermal thickness, with a mean difference of 29 percent between pretreatment and post-treatment values, and a decrease in the thickness between the stratum basale and the stratum granulosum, with a mean difference of 31 percent. The degree of psoriasis activity also improved significantly and the number of keratinocytes stained with Ki-67 decreased significantly, suggesting that one of the effects of chondroitin sulfate is directed on keratinocyte hyperproliferation. Finally, all patients but three had orthokeratotic keratinization after treatment with chondroitin sulfate.
Psoriasis is a chronic immune-mediated disease that frustrates patients and, all too often, the dermatologists who treat them. Advances in the understanding of the autoimmune-cutaneous reaction that is believed to play a causative role in the development of skin lesions in psoriasis [13], and the recognition of T cells as primary mediators of psoriasis pathogenesis [14] have led to the identification of potential targets for therapeutic intervention, including biologic therapies [15, 16, 17]. However, important developments in the history of psoriasis pharmacotherapy have largely occurred by chance in association with serendipitous observations in single patients [14], such as the use of methotrexate, deltanoids (active form of vitamin D and its analogues), cyclosporin and, most recently, tumor necrosis factor α (TNF-α) inhibitors [18]. We treated a group of patients with bilateral knee osteoarthritis with chondroitin sulfate, a symptomatic slow-acting drug for osteoarthritis. These patients also had a mean 26-year history of severe psoriasis and shortly after oral treatment with the drug, their psoriasis dramatically improved in appearance. Clinical improvement was confirmed by histologic studies. To our knowledge this is the first reported serendipitous finding of successful chondroitin sulfate therapy in psoriasis. This observation has the clear limit of the small sample of patients.
Chondroitin sulfate belongs to the group of glycosaminoglycans, which are linear polysaccharides located in the extracellular matrix and on the cell surface. Studies of metabolically labeled human keratinocytes with 3[H]glucosamine have identified the components of cell-surface glycosaminoglycans as hyaluronic acid (54 %), heparin sulfate (33 %), and chondroitin sulfate (13 %) [19]. Although the physiological roles and interactions of glycosaminoglycans with other molecules remain unclear, some mechanisms of action may account for the effect of chondroitin sulfate in psoriasis. For example, it has been shown that several sulfated polysaccharides, including chondroitin sulfates B and C, can act as inhibitors of amphiregulin-mediated autonomous proliferation in human epidermal keratinocytes [20]. Over-expression of some keratinocyte growth factors (e.g., amphiregulin) leads to the development of a psoriasis-like phenotype in otherwise healthy skin [21]. On the other hand, chondroitin polysulfate (a semi-synthetic over-sulfated chondroitin sulfate) enhanced the production of native hyalunorate glycosaminoglycans in human dermal fibroblasts in a dose-dependent manner [22]. Recently, using four novel antichondroitin sulfate antibodies, alterations in the distribution of chondroitin sulfate in psoriasis have been detected [23]. The observation of the beneficial effect of chondroitin sulfate by serendipity may be consistent with the restoration of chondroitin sulfate alterations in the papillary dermis and basal keratinocytes [23].
In view of the potential interest of chondroitin sulfate for the treatment of psoriasis, a placebo controlled study in patients with psoriasis must be performed to assess the impact of treatment on the patient's quality of life [24].
Acknowledgments: We thank Prof. Dr. Patrick du Souich, Department of Pharmacology, University of Montreal, Quebec, Canada, for his valuable contribution in the discussion of results of the study, Ms. Gemma Cumelles for her help in the follow-up of patients, and Dr Marta Pulido for editing the manuscript and editorial assistance.
Conflict of interest statement: Please, note that three of the authors are full employers as Director (J.V.) and staff members (E.M. and M.H.) of the Unit of Clinical Research of the Scientific and Medical Department of Bioibérica, S.A., which is the pharmaceutical company of the study drug (Condro∙san®). None of the authors had received honoraria from Bioibérica, S.A., for the participation in the study.
References
1. Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JW, Dieppe P, Gunther K, Hauselmann H, Herrero-Beaumont G, Kaklamanis P, Lohmander S, Leeb B, Lequesne M, Mazieres B, Martin-Mola E, Pavelka K, Pendleton A, Punzi L, Serni U, Swoboda B, Verbruggen G, Zimmerman-Gorska I, Dougados M; Standing Committee for International Clinical Studies Including Therapeutic Trials ESCISIT. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2003;62:1145-55. PubMed.2. Hardingham T. Chondroitin sulfate and joint disease. Osteoarthritis Cartilage 1998;6 (Suppl A):3-5. PubMed
3. Ronca F, Palmieri L, Panicucci P, Ronca G. Anti-inflammatory activity of chondroitin sulfate. Osteoarthritis Cartilage 1998;6(Suppl A):14-21. PubMed
4. Maneiro E, Fernandez Sueiro J, et al. Efecto del condroitin sulfato sobre la produccion de oxido nitrico por los condrocitos humanos artrosicos. Rev Esp Reumatol 2001;28:12-17.
5. Bali JP, Cousse H, Neuzil E. Biochemical basis of the pharmacologic action of chondroitin sulfates on the osteoarticular system. Semin Arthritis Rheum. 2001;31:58-68. PubMed
6. Uebelhart D, Malaise M, Marcolongo R, DeVathaire F, Piperno M, Mailleux E, Fioravanti A, Matoso L, Vignon E. Intermittent treatment of knee osteoarthritis with oral chondroitin sulfate: a one-year, randomized, double-blind, multicenter study versus placebo. Osteoarthritis Cartilage. 2004 Apr;12(4):269-76. PubMed
7. Mazieres B, Combe B, Phan Van A, Tondut J, Grynfeltt M. Chondroitin sulfate in osteoarthritis of the knee: a prospective, double blind, placebo controlled multicenter clinical study. J Rheumatol 2001;28:173-81. PubMed.
8. Leeb BF, Schweitzer H, Montag K, Smolen JS. A metaanalysis of chondroitin sulfate in the treatment of osteoarthritis. J Rheumatol 2000;27:205-11. PubMed.
9. Morreale P, Manopulo R, Galati M, Boccanera L, Saponati G, Bocchi L. Comparison of the antiinflammatory efficacy of chondroitin sulfate and diclofenac sodium in patients with knee osteoarthritis. J Rheumatol. 1996 Aug;23(8):1385-91. PubMed.
10. du Souich P, Verges J. Simple approach to predict the maximal effect elicited by a drug when plasma concentrations are not available or are dissociated from the effect, as illustrated with chondroitin sulfate data. Clin Pharmacol Ther. 2001 Jul;70(1):5-9. Review. No abstract available. PubMed.
11. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, Christy W, Cooke TD, Greenwald R, Hochberg M, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986 Aug;29(8):1039-49. PubMed.
12. Verges J, Montell E, Herrero M, Perna C, Cuevas J, Perez M, Moller I. Mejoria clinica y anatomopatologica de la psoriasis en pacientes con artrosis tratados con condroitin sulfato: descripcion de tres casos. Med Clin (Barc). 2004 Nov 27;123(19):739-42. PubMed.
13. Menter MA, Krueger GC, Feldman SR, Weinstein GD. Psoriasis treatment 2003 at the new millennium: position paper on behalf of the authors. J Am Acad Dermatol. 2003 Aug;49(2 Suppl):S39-43. No abstract available. PubMed.
14. Gniadeck R, Zachariae C, Calverley M. Trends and developments in the pharmacological treatment of psoriasis. Acta Derm Venereol. 2002;82(6):401-10. PubMed.
15. Gordon KB, McCormick TS. Evolution of biologic therapies for the treatment of psoriasis. Skinmed. 2003 Sep-Oct;2(5):286-94. PubMed.
16. Nickoloff BJ, Nestle FO. Recent insights into the immunopathogenesis of psoriasis provide new therapeutic opportunities. J Clin Invest. 2004 Jun;113(12):1664-75. PubMed.
17. Walsh SR, Shear NH. Psoriasis and the new biologic agents: interrupting a T-AP dance. CMAJ. 2004 Jun 22;170(13):1933-41. PubMed.
18. Oh CJ, Das KM, Gottlieb AB. Treatment with anti-tumor necrosis factor alpha (TNF-alpha) monoclonal antibody dramatically decreases the clinical activity of psoriasis lesions. J Am Acad Dermatol. 2000 May;42(5 Pt 1):829-30. PubMed.
19. Brown KW, Parkinson EK. Glycoproteins and glycosaminoglycans of cultured normal human epidermal keratinocytes. J Cell Sci. 1983 May;61:325-38. PubMed.
20. Cook PW, Mattox PA, Keeble WW, Shipley GD. Inhibition of autonomous human keratinocyte proliferation and amphiregulin mitogenic activity by sulfated polysaccharides. In Vitro Cell Dev Biol. 1992 Mar;28A(3 Pt 1):218-22. PubMed.
21. Cook PW, Piepkorn M, Clegg CH, , et al. Transgenic expression of the human amphiregulin gene induces a psoriasis-like phenotype. J Clin Invest. 1997 Nov 1;100(9):2286-94. PubMed.
22. Mitsuyama S, Tanaka S, Urushizaki F, Yoshida T, Ito A. Mori Y. Effects of glycosaminoglycan polysulfate on extracellular matrix metabolism in human skin cells. Res Commun Chem Pathol Pharmacol. 1994 Feb;83(2):179-93. PubMed.
23. Smetsers TF, van de Westerlo EM, ten Dam GB, Overes IM, Schalkwijk J, van Muijen GN, van Kuppevelt TH. Human single-chain antibodies reactive with native chondroitin sulfate detect chondroitin sulfate alterations in melanoma and psoriasis. J Invest Dermatol. 2004 Mar;122(3):707-16. PubMed.
24. Mazzotti E, Picardi A, Sampogna F, Sera F, Pasquini P, Abeni D; IDI Multipurpose Psoriasis Research on Vital Experiences study group. Sensitivity of the Dermatology Life Quality Index to clinical change in patients with psoriasis. Br J Dermatol. 2003 Aug;149(2):318-22. PubMed.
© 2005 Dermatology Online Journal